
Insulin Resistance, Diabetes and Lipedema
How insulin signaling, insulin resistance and blood sugar regulation may help us understand one important metabolic layer of lipedema.

LipedemaScience is where I try to make complex lipedema science understandable without making it simple in the wrong way. This article is part of that work. It is written for women with lipedema who want to understand their bodies more deeply, and for those who have started wondering whether insulin, blood sugar, inflammation and adipose tissue biology may be part of their own symptom picture.
As a food scientist and nutritionist, I have always been interested in how food interacts with the body. Not only in the simple sense of calories, protein, carbohydrates and fat, but in the deeper biological sense. How does food change hormones. How does it affect inflammation. How does it influence the gut microbiome, the immune system, the blood vessels and the way our cells communicate with each other.
When I studied human nutrition, much of the focus was on lifestyle related diseases. We learned about type 1 diabetes, type 2 diabetes and gestational diabetes. We learned about blood sugar regulation, insulin treatment, pregnancy related glucose intolerance and the long term complications of diabetes. But I do not remember insulin resistance being explained to me as its own important state in the body.
That is why I still remember the first time one of my readers asked me about insulin resistance and lipedema. This was a couple of years ago, and I had to admit that I did not really know what to answer. It was not because I had never studied metabolism. I had. It was not because I did not understand glucose or diabetes. I did. But insulin resistance as a separate, quiet, early metabolic dysfunction was not something I had spent much time thinking about in relation to lipedema.
To be honest, I love getting questions like that from this community. They make me grow. They force me to go back to the biology, read more, think more and sometimes admit that I do not know enough yet. Even with a background in human nutrition and food science, you never become an expert on everything. The body is too complex for that. And in lipedema, there are still so many unanswered questions.
That curiosity is one of the reasons I started looking more closely at insulin resistance. I wanted to understand how it differs from type 1 diabetes, type 2 diabetes and gestational diabetes. I wanted to understand what actually happens inside the cells when insulin works normally, and what happens when the cells stop responding properly.
This also became personal in a different way because two of my close friends from university have lived experience with different forms of disturbed glucose metabolism. One of my very good friends has type 1 diabetes. She needs insulin and tracks her blood sugar every day. Another friend, who also has a background in both human nutrition and food science, developed gestational diabetes during pregnancy, even though she was healthy, active and highly knowledgeable about nutrition. In her case, it was not a story of poor lifestyle. It was a story of biological vulnerability meeting the metabolic stress test of pregnancy.
We have spent many hours discussing how blood sugar behaves in real life. Not only in theory, but in actual bodies. Both of them have told me how certain foods that are often considered healthy can still give surprisingly high blood sugar responses. Oatmeal is one example. In theory, oatmeal should usually give a slower rise in blood sugar than refined white bread or sugary cereal. But in real people, the response can vary a lot. When oatmeal is eaten alone, it may spike blood sugar more than expected. When it is combined with protein or fat, the response can look quite different, because protein and fat slow down how quickly the carbohydrate is absorbed. The protein and fat are doing the real work.
That was also something we saw when I studied nutrition. In one class, we were divided into groups and tested how different meals affected our bodies. My group had to eat white bread with jam. I still remember how awful I felt afterwards. It was not my kind of breakfast or lunch at all. Another group ate eggs and bacon, a very old style low carbohydrate meal. Another had whole grain bread with ham, cheese and vegetables. Another had a smoothie. The point was not that one meal is universally good and another is universally bad. The point was that food is not only food. Food is information. The body reads it through glucose, insulin, gut hormones, satiety signals, inflammatory responses and energy metabolism.
This is why insulin resistance has become such an interesting topic for me in relation to lipedema. Not because I believe every woman with lipedema has insulin resistance. I do not. The evidence is not that simple, and the lipedema population is not metabolically identical from person to person. Some women with lipedema are insulin resistant. Some are not. Some have normal blood sugar for years. Some have PCOS, gestational diabetes, type 2 diabetes or a family history that makes the picture more complicated. Some have clear symptoms after certain foods, while others do not.
But I do think insulin resistance is something many of us should at least understand. Not as a diagnosis we give ourselves, but as a possible layer in the larger lipedema picture.

In my own case, I once asked my GP to check whether I could have signs of insulin resistance. We tested glucose and other markers. There were some signs that made me wonder, but not enough to clearly confirm it. That is part of the challenge. Insulin resistance can be tricky to detect in a regular doctor’s appointment, especially if fasting glucose and HbA1c are still normal. The body can compensate for a long time by producing more insulin. From the outside, everything may look fine, while the pancreas is working harder in the background.
Because of that, I keep it in the back of my mind. I may have some degree of insulin resistance. I may not. But if the lifestyle measures that support insulin sensitivity also support inflammation, energy levels, hormonal balance and long term metabolic health, then I would rather take them seriously than ignore them completely.
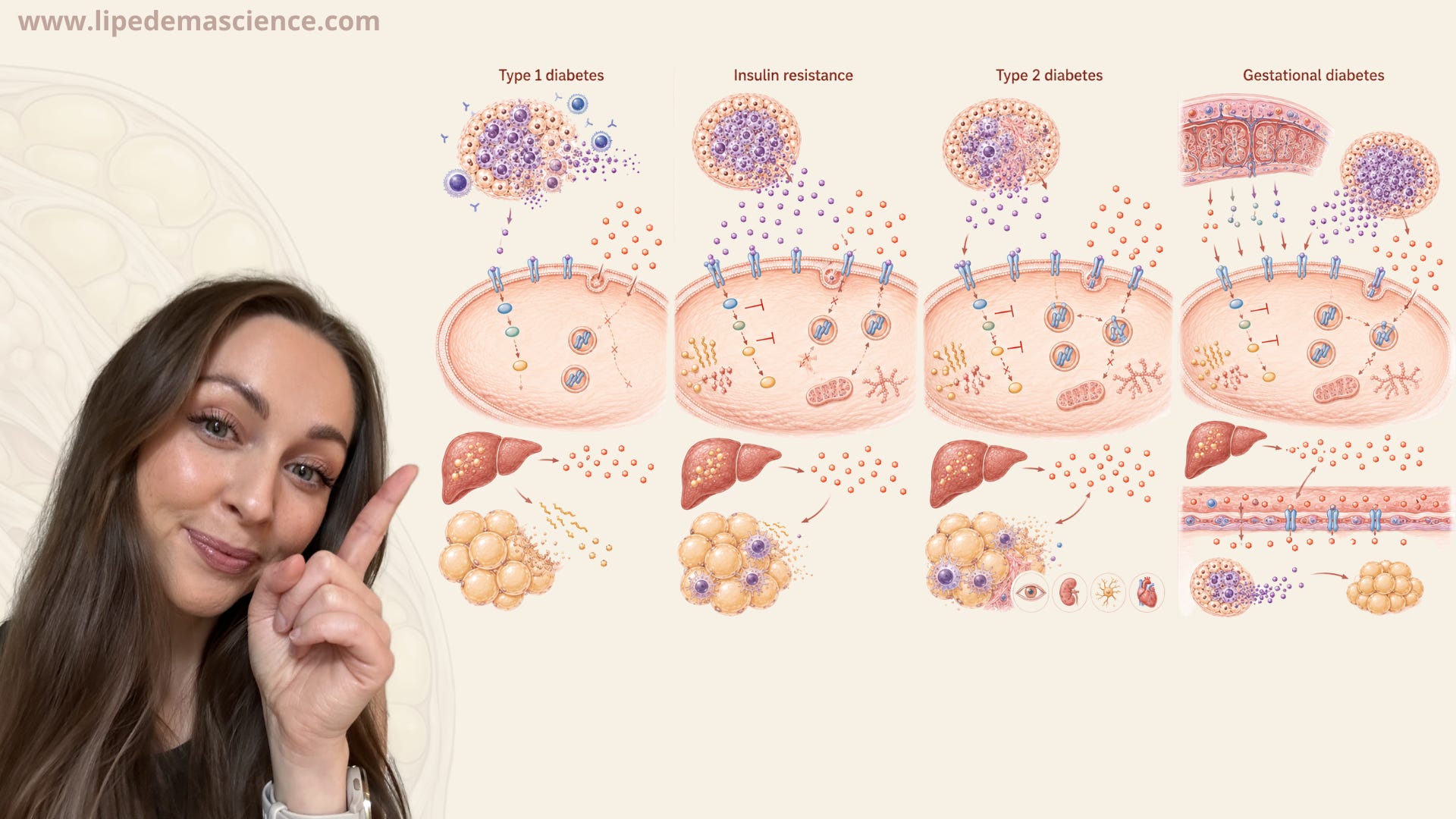
This article is my attempt to explain the basics clearly. What insulin normally does. What happens in type 1 diabetes. What insulin resistance means. How type 2 diabetes develops. Why gestational diabetes can happen even in healthy women. And finally, why this matters for lipedema.
At the center of all of this is one hormone.
Insulin.
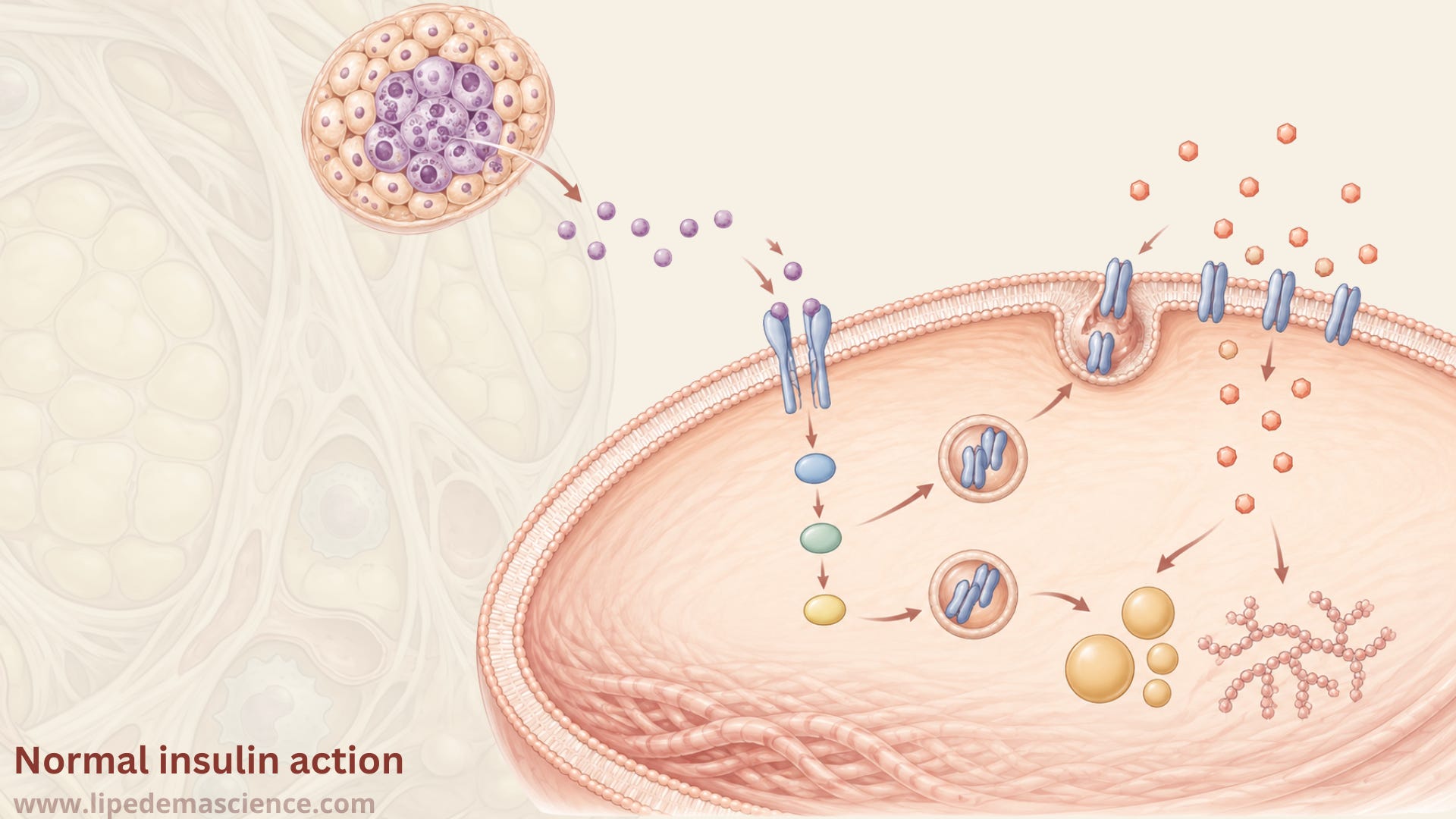
Insulin is often described as the hormone that lowers blood sugar, but that is only part of the story. Insulin is really one of the body’s main storage signals. It tells cells that energy is available. It tells muscle and fat cells to take up glucose. It tells the liver to stop producing glucose and start storing energy. It tells fat tissue to reduce the release of fatty acids. In other words, insulin helps move the body from a fasting state into a fed state.
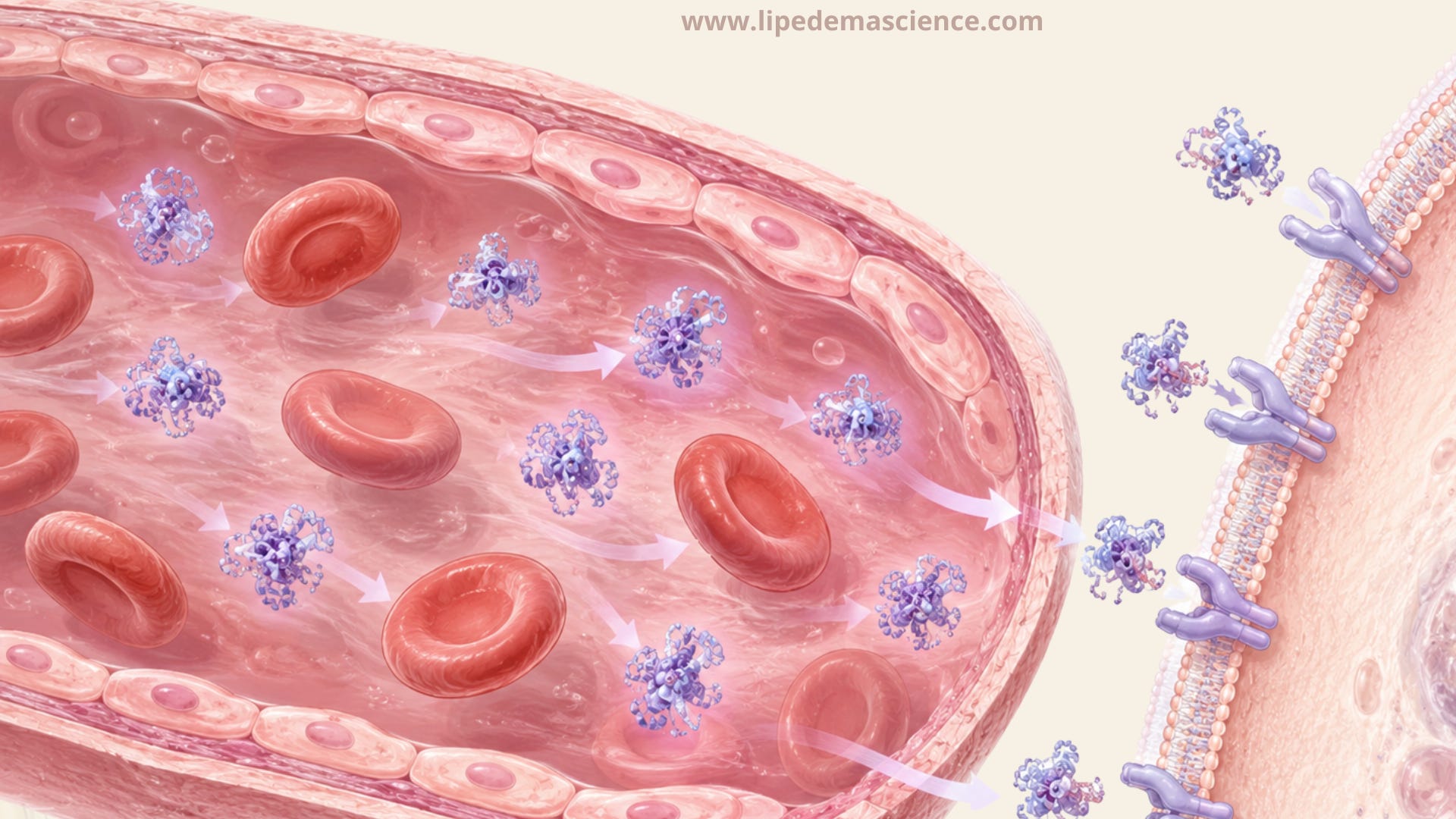
After we eat carbohydrates, glucose rises in the blood. The pancreas senses this and releases insulin from the beta cells in the islets of Langerhans. Insulin then travels through the bloodstream and binds to insulin receptors on target cells, especially in muscle, fat tissue and the liver.
On the cell surface, the insulin receptor works like a molecular switch. When insulin binds, the receptor becomes activated and starts a chain reaction inside the cell. This involves proteins such as IRS, PI3K and Akt. The names are technical, but the concept is not. Insulin knocks on the door, the receptor hears the knock, and the cell starts moving glucose transporters toward the surface.
In muscle and fat cells, one of the most important results is that GLUT4 transporters move from storage vesicles inside the cell to the cell membrane. These GLUT4 transporters act like doors for glucose. When they reach the membrane, glucose can enter the cell more efficiently. In muscle, that glucose can be used for energy or stored as glycogen. In fat tissue, insulin promotes storage and reduces the release of fatty acids. In the liver, insulin suppresses glucose production and promotes glycogen synthesis and fat production.
When this system works well, blood sugar rises after a meal and then comes back down in a controlled way. The pancreas releases insulin, the cells respond, glucose is taken up, and the body returns toward balance.
But when this system fails, it can fail in different ways.
The first way is that the body does not produce enough insulin.
This is the core problem in type 1 diabetes.
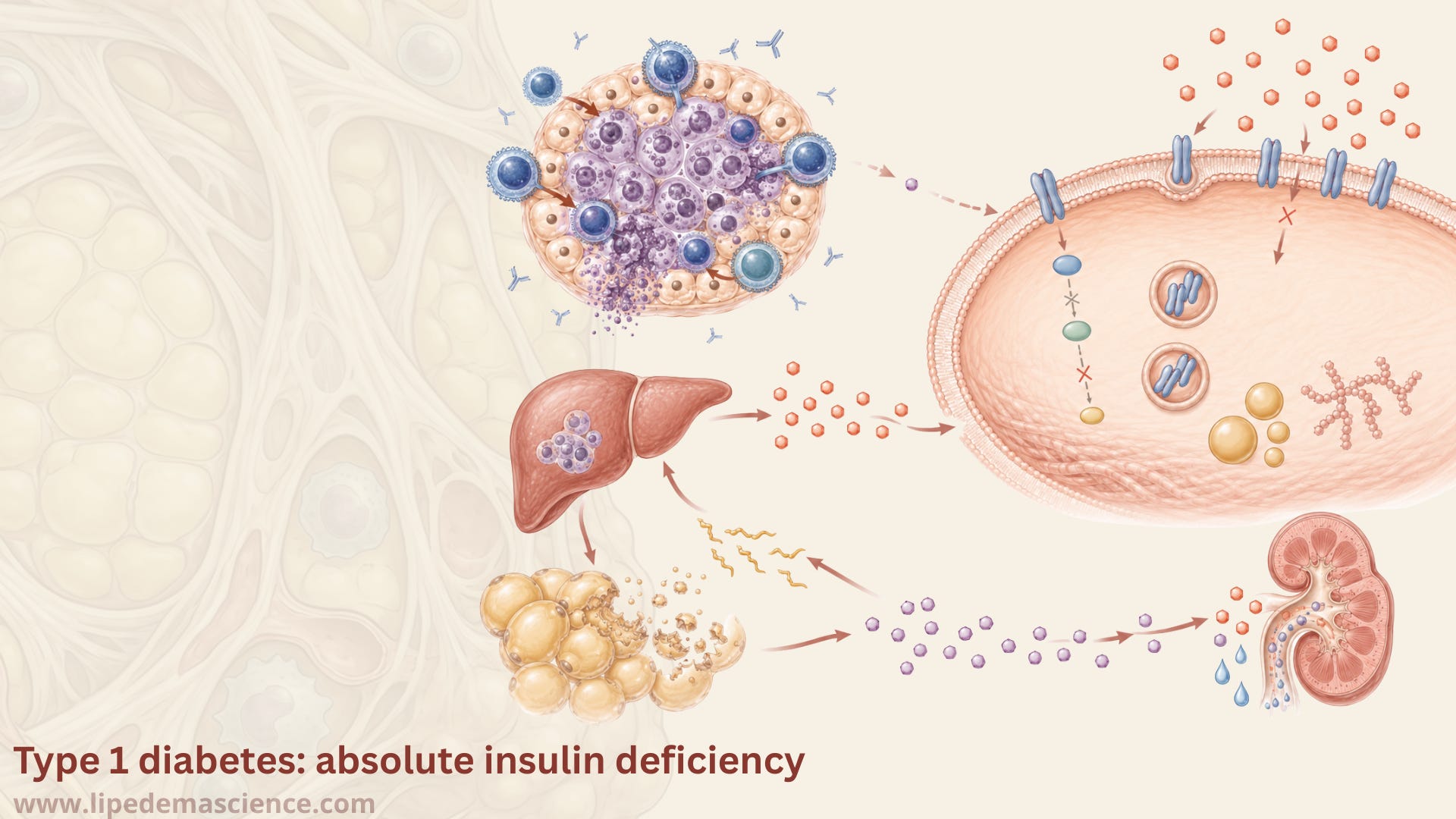
Type 1 diabetes is an autoimmune disease. The immune system attacks and destroys the insulin producing beta cells in the pancreas. This can happen gradually, and autoantibodies may be detectable before symptoms appear. Eventually, the body loses the ability to make enough insulin.
The key point is that type 1 diabetes is not primarily a problem of the cells ignoring insulin. It is a problem of insulin being absent or severely deficient. The signal is missing.
Without insulin, muscle and fat cells cannot take up glucose normally. At the same time, the liver behaves as if the body is fasting, even when blood sugar is already high. It continues to release glucose into the bloodstream. This creates the strange and dangerous situation where there is too much glucose in the blood, but many cells cannot access it properly.
Because insulin normally suppresses fat breakdown, lack of insulin also allows fat tissue to release large amounts of fatty acids. The liver converts some of these fatty acids into ketones. In untreated type 1 diabetes, ketones can accumulate and cause diabetic ketoacidosis, a life threatening acidification of the blood.
This is why people with type 1 diabetes need insulin. Not as a lifestyle tool, not as a temporary support, but as a life sustaining treatment.
Insulin resistance is different.
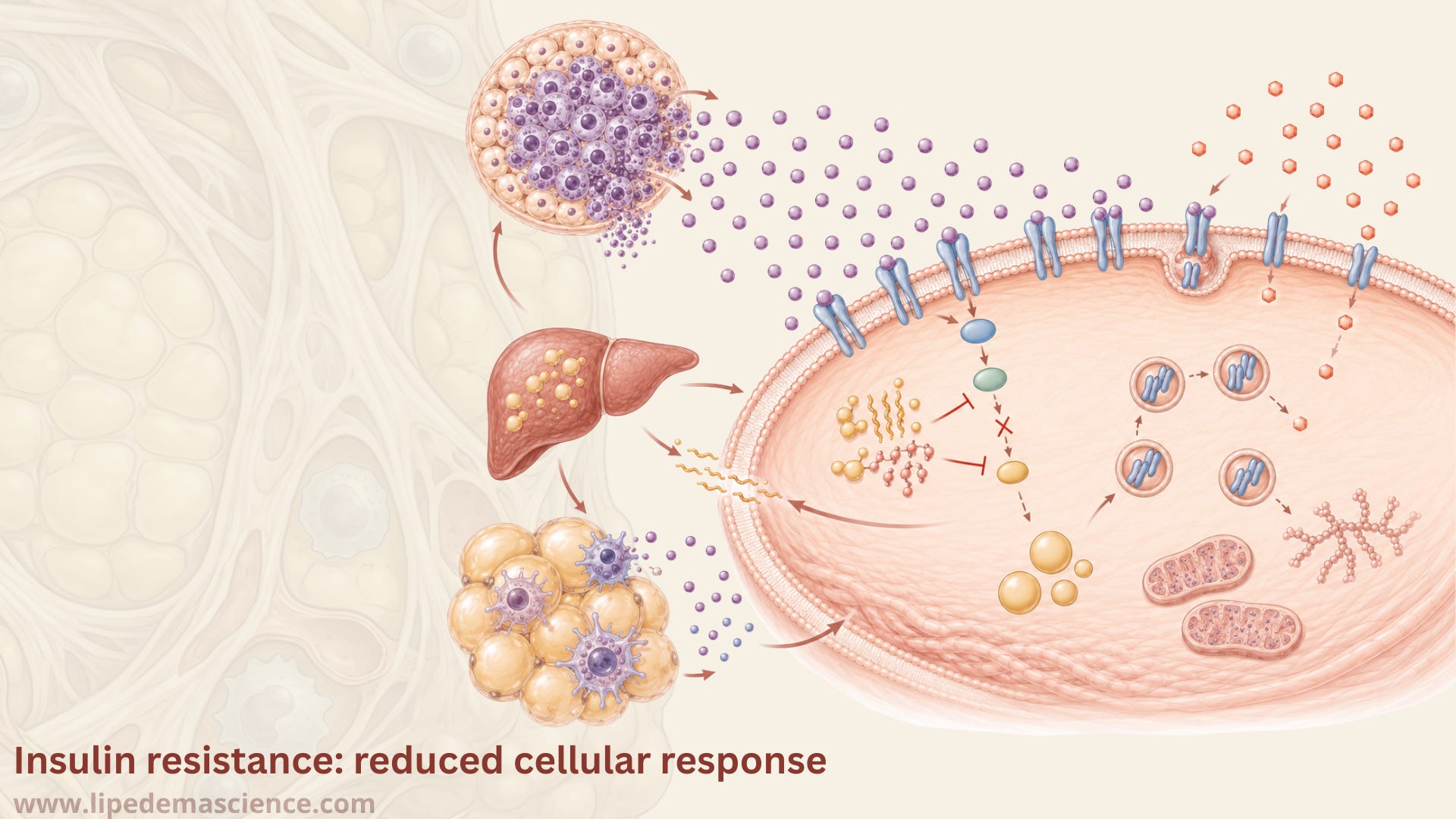
In insulin resistance, insulin is present. Often, especially in the early stages, there is a lot of it. The problem is that the cells do not respond properly. The signal is there, but the cells are less sensitive to it.
This can happen in muscle, liver and fat tissue. In muscle, glucose uptake becomes less efficient. In the liver, insulin fails to suppress glucose production properly. In fat tissue, insulin’s ability to regulate fat storage and fat release becomes disturbed. The pancreas tries to compensate by producing more insulin. For a while, this can keep blood sugar normal.
This is one reason insulin resistance can be silent. If a doctor only checks fasting glucose or HbA1c, everything may look acceptable for a long time. But behind the scenes, the body may be maintaining normal glucose by producing more insulin than it should need.
At the cellular level, insulin resistance involves problems in the insulin signaling pathway. Instead of a clean signal from the insulin receptor through IRS, PI3K and Akt, the signal becomes weaker or disrupted. Lipid molecules can accumulate in places where they do not belong, especially in muscle and liver. Inflammatory signals can interfere with insulin signaling. Mitochondrial dysfunction may also play a role. Adipose tissue inflammation can contribute through cytokines and immune cell activity.
This is where things become interesting for lipedema.
Lipedema is not simply obesity. It is a disease of abnormal, painful, often fibrotic adipose tissue, with vascular, lymphatic, inflammatory and hormonal features. The affected tissue does not behave like ordinary fat tissue. Many women describe swelling, heaviness, pain, easy bruising and a disproportionate fat distribution that behaves stubbornly. When women with lipedema lose weight, the affected areas, usually the legs and hips, often shrink far less than the rest of the body, so the disproportion tends to remain. This does not mean weight loss is pointless. It still reduces fat, it can ease pain and it may slow progression. It simply means you usually cannot slim the affected areas selectively in the way diet culture promises. Research increasingly points toward altered microcirculation, connective tissue remodeling, immune activity and adipose tissue dysfunction.
Because insulin is one of the most important hormones acting on fat tissue, it makes sense to ask whether insulin resistance could matter in lipedema. But we have to ask that question carefully.
It would be too simplistic to say that lipedema is caused by insulin resistance. I do not believe the evidence supports that. In fact, some of the most careful studies suggest something that surprises people: when researchers compare women with lipedema to women of the same body size without lipedema, the women with lipedema often have better insulin sensitivity, not worse. I think that is a genuinely important point, because it pushes back against the lazy assumption that larger legs must mean a broken metabolism. It would also be too simplistic, though, to say that insulin resistance is irrelevant. The more reasonable position is that insulin resistance may be one contributing factor in some women with lipedema, especially when lipedema overlaps with weight gain, PCOS, a history of gestational diabetes, central adiposity, inflammatory symptoms or metabolic syndrome markers.
This distinction matters because women with lipedema are often told two opposite but equally unhelpful things. One is that everything is their fault and they should simply eat less. The other is that metabolism does not matter at all because lipedema fat is different. I think both positions are too flat.
Lipedema fat is different. That does not mean the rest of metabolism becomes irrelevant.
The body is one connected system. Fat tissue communicates with immune cells, blood vessels, hormones, the gut, the liver, skeletal muscle and the brain. If insulin resistance is present, it may influence inflammation, fluid retention, energy levels, hunger signals, fat storage, lipid metabolism and vascular function. It may not explain lipedema itself, but it could influence how the disease feels and progresses in some women.
Type 2 diabetes develops when insulin resistance and beta cell failure come together.
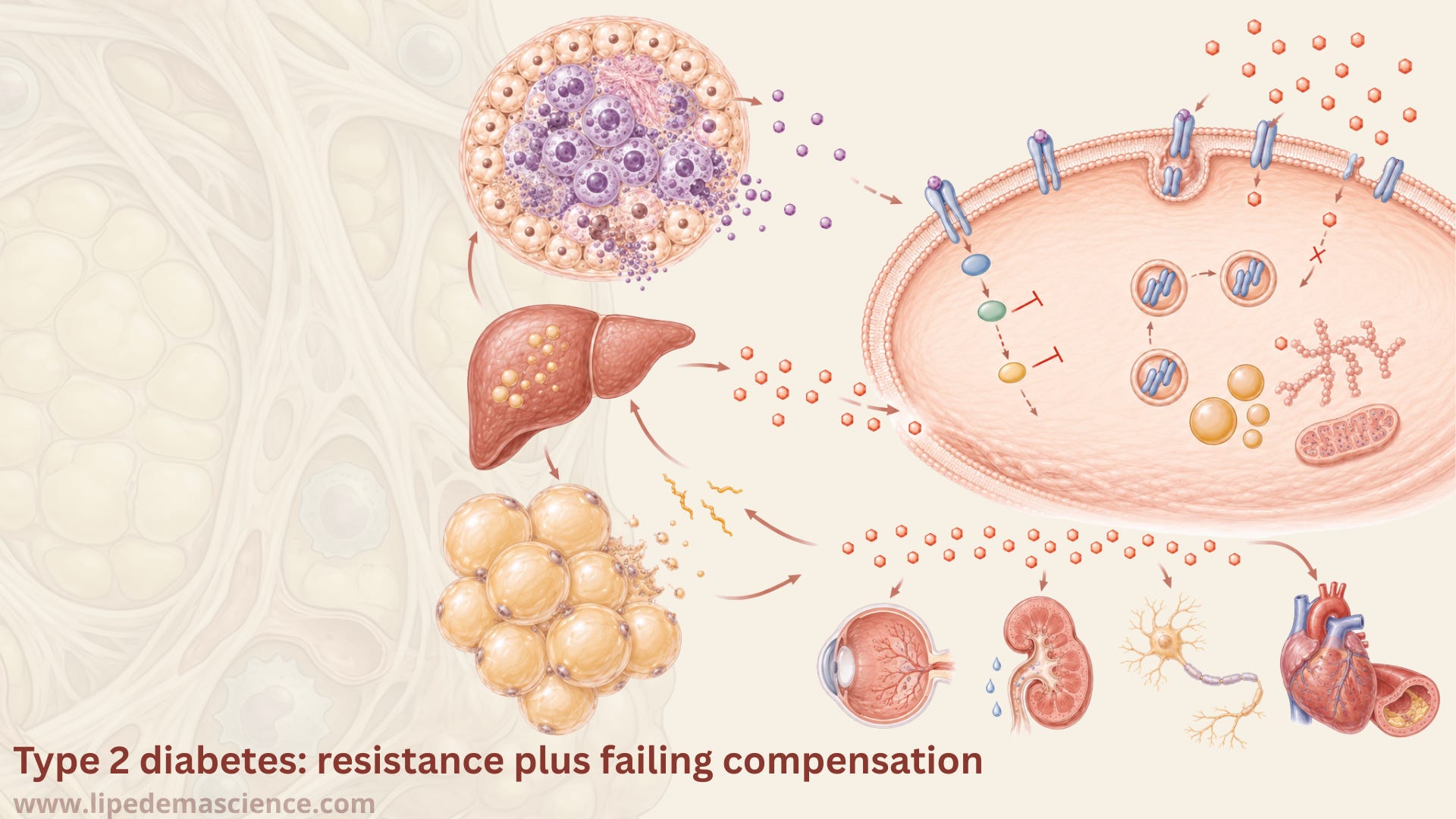
In the early phase, the pancreas compensates by producing more insulin. This can work for years. But over time, the beta cells may no longer keep up. Chronic high glucose, high fatty acids, inflammation and stress inside the beta cells can reduce their function. When insulin production is no longer enough to overcome the resistance, blood sugar rises. That is when prediabetes or type 2 diabetes becomes visible through standard tests.
The important difference between insulin resistance and type 2 diabetes is therefore compensation. In insulin resistance, the pancreas may still be able to compensate. In type 2 diabetes, compensation is no longer sufficient.
This also means that type 2 diabetes usually develops gradually. It is not one sudden switch. It is often a long process where the body works harder and harder to maintain normal glucose until it no longer can.
Gestational diabetes is another version of this story, but with pregnancy as the stress test.
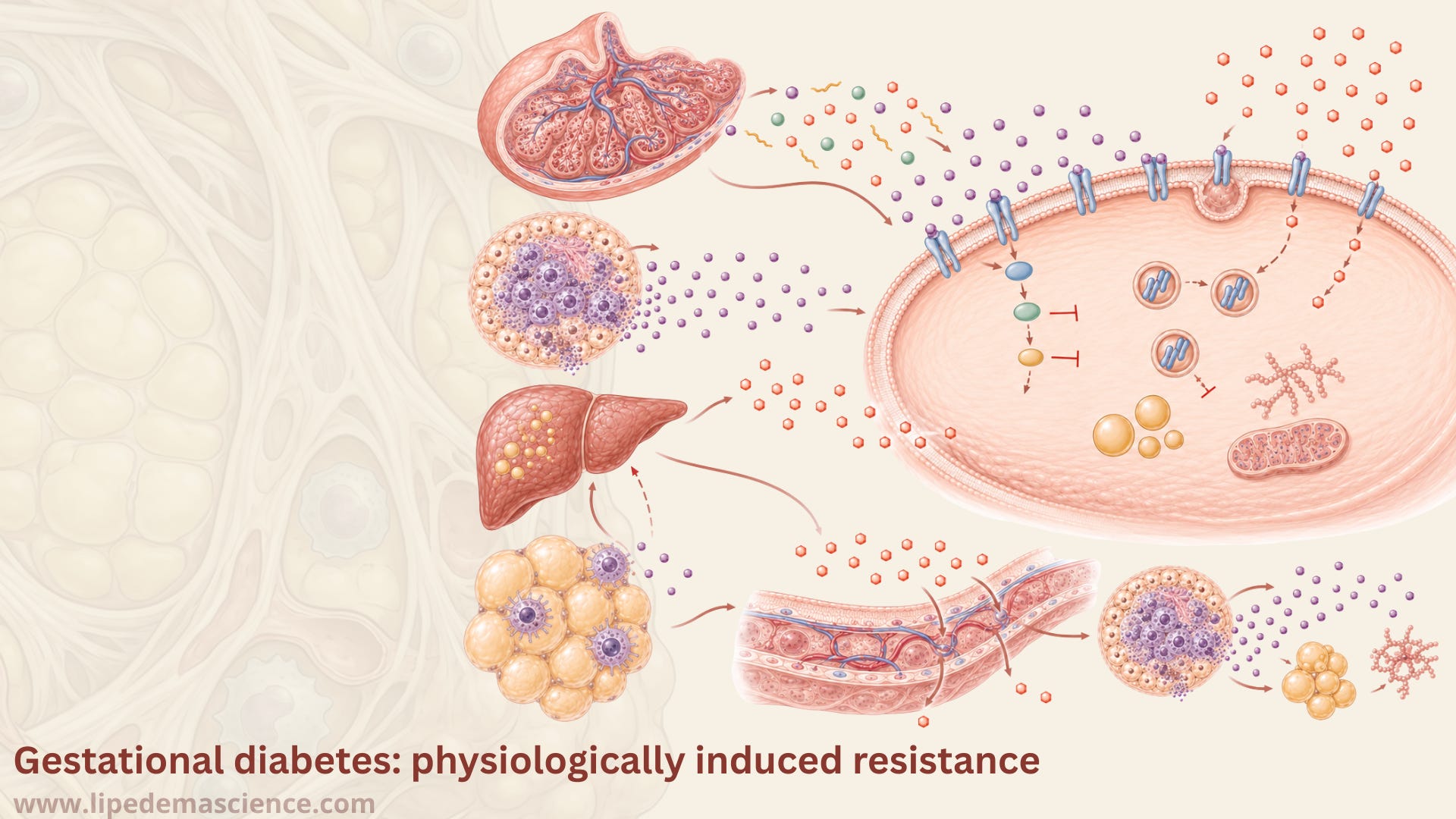
During pregnancy, the placenta produces hormones that naturally make the mother more insulin resistant. This is not a mistake. It is part of normal pregnancy physiology. By making the mother’s tissues slightly more insulin resistant, more glucose remains available for the growing fetus.
Most women compensate by producing more insulin. Gestational diabetes occurs when the beta cells cannot compensate enough for the pregnancy induced insulin resistance. This can happen even in women who are active, healthy and knowledgeable about food. Pregnancy reveals a metabolic vulnerability that may not have been obvious before.
That is why I think gestational diabetes is often misunderstood. It is not simply a sign that someone did something wrong. It can be a sign that the body was pushed into a state where its insulin producing capacity was not enough for the demand.
For women with lipedema, this is relevant because many report that lipedema begins or worsens around hormonal transitions such as puberty, pregnancy, perimenopause or menopause. These are also times when insulin sensitivity, sex hormones, inflammation and fat distribution can change. We do not yet have all the answers, but the overlap is biologically interesting. The current thinking is not that women with lipedema have abnormal hormone levels in their blood, but that the affected tissue itself seems unusually sensitive to normal hormonal shifts.
So what can we actually do with this knowledge.
First, I think we need to stop seeing blood sugar as only a diabetes issue. Blood sugar regulation is part of metabolic health. Insulin sensitivity is part of metabolic health. And metabolic health may matter in lipedema even when a person is not diabetic.
Second, I think we need to become more curious about individual responses. One woman may tolerate oatmeal well. Another may get a strong glucose response unless she combines it with protein and fat. One woman may feel better on a Mediterranean style diet with legumes, whole grains, fish, olive oil and vegetables. Another may need a lower carbohydrate approach to reduce symptoms. One may react strongly to refined sugar with swelling or pain. Another may not notice an immediate effect.

This does not mean everything is random. It means human metabolism is individual. In practice, the lifestyle measures that improve insulin sensitivity are not extreme. Strength training is one of the most powerful tools because skeletal muscle is a major site of glucose disposal. Walking after meals can reduce post meal glucose rises. Protein and fiber can slow digestion and improve satiety. Replacing refined carbohydrates with less processed foods can reduce glucose peaks. Sleep matters. Stress matters. Alcohol can matter. Omega 3 rich fish, colorful plants, fermented foods and anti inflammatory dietary patterns may support the broader inflammatory environment. None of this means that lifestyle cures lipedema. It does not. I am very clear about that. But lifestyle can still matter.
For me, the most useful mindset is not control. It is support. I am not trying to punish my body into behaving. I am trying to understand what kind of environment gives my body the best chance to function well.
This is also why I have decided to use more of my own background in human nutrition and food science in LipedemaScience going forward. I have worked with the gut microbiome at DNA level and molecular level. I have worked with inflammation, intestinal permeability and what people often call leaky gut. I have spent years in laboratories. I have worked as a nutrition coach. I have worked with lifestyle related diseases. I know enough to see that lipedema cannot be reduced to nutrition, but I also know enough to see that nutrition should not be excluded from the conversation.
We need a more mature discussion..
A discussion where we can say that lipedema is a real disease, not a failure of willpower.
A discussion where we can say that surgery can reduce diseased tissue and improve symptoms, but it is not a metabolic reset button for everyone.
A discussion where we can say that insulin resistance may be relevant for some women, without turning it into another thing women are blamed for.
A discussion where we can say that food can be powerful, without pretending it is magic.
If you are reading this and wondering whether you might have insulin resistance, the best next step is not to panic or self diagnose. It is to talk to a healthcare professional and ask about appropriate testing. Fasting glucose and HbA1c can be useful, but they may not always show early insulin resistance. Depending on the situation, fasting insulin, C peptide, lipid profile, waist measures, blood pressure, oral glucose tolerance testing or HOMA IR may be discussed. These are screening tools rather than a single definitive test, and what they mean depends on the whole picture. The right tests depend on your history, symptoms and risk factors.
And if everything looks normal, that is still useful information. Not every woman with lipedema is insulin resistant. We need to allow for that too.
The main thing I hope you take from this article is that insulin is not only about diabetes. It is about how the body handles energy. It is about communication between the pancreas, liver, muscle, fat tissue and blood vessels. It is about whether the cells hear the signal they are supposed to hear.
In type 1 diabetes, the insulin signal is missing.
In insulin resistance, the signal is present, but the cells respond poorly.
In type 2 diabetes, insulin resistance is combined with beta cells that can no longer compensate enough.
In gestational diabetes, pregnancy creates a natural insulin resistant state, and diabetes appears when the body cannot compensate sufficiently.
For lipedema, the question is not whether insulin resistance explains everything. It does not. The question is whether insulin resistance may be one important metabolic layer for some of us. I think that question deserves more attention, more research and more careful discussion.
And I think many women with lipedema deserve to understand this biology before they are told that everything is either their fault or completely outside their influence. Neither is true. The body is more complex than that.
LipedemaScience exists because women with lipedema deserve access to deep, serious and understandable science about their own bodies. My goal is to translate research and physiology into articles that make you feel more informed, not more confused, and more respected, not blamed. If you want to keep learning about lipedema through a scientific but human lens, including metabolism, hormones, inflammation, pain, surgery, nutrition, fibrosis, lymphatics and the lived reality of this disease, you can subscribe to LipedemaScience. Paid subscriptions make it possible for me to spend the time needed to read the research properly, connect the dots carefully and build a knowledge platform that treats lipedema with the seriousness it deserves.
Thank you for this information. As an insulin diabetic I have often wondered if there may be some connection. Your article is extremely helpful. Understanding some contributors to lipedema is great knowledge. I have had a conversation with my endocrinologist she was not aware of a connection. I gave her some information that I received from Lipedema Australia and she was happy with that. I also have connective tissue disorder so when I go to my appointment tomorrow, I will give them the same information as I have told them years ago about my lipedema. Your research and knowledge is amazing. Thank you and keep up the great work you give us inspiration.
TGLUT Translocation GLUT-4 and -12 together can have 10X capacity of other 11 glucose transporters combined. Designed as a gated response on eating, must these protein receptors must physically move to surface for receipt of glucose from glucose-insulin carrier in blood. If not at surface, no pickup (think short order cook at pickup window). If not received into cells for energy burning, pancreas signals for more insulin already not the problem causing excess glucose to be stored as fat and inhibiting fat burning. The 10 year insulin resistance cycle from post-parandial high glucose through pre-diabetic to diabetic. Missed by most endocrinologists by failure to test fasting insulin which can suppress glucose into normal range. Insulin resistance calculation HOMa-IR calculation (safer than clinical glucose tolerance test), inputs fasting glucose and fasting insulin. Lymphatic disorders more challenging for this uptake and increased insulin sensitivity due to larger limbs and fibrosis, leaky lymph forming glycoaminoglycans. The latter useful for fascia structure but lymph no long fluid and in exit channel causing eventual progression and fibrosis (reversible with a lot of work). Easier the earlier detection as is insulin resistance.