
Lipedema Is Not Obesity — But the Two Can Coexist
Understanding how altered adipose tissue, fluid retention, and connective tissue changes in lipedema can increase body weight without the metabolic mechanisms that define obesity.

A recent paper published in JPRAS Open in 2026 offers a useful entry point into this discussion. It is a narrative review, not a systematic review and not an intervention study. That distinction matters. A narrative review can be valuable for summarizing themes in the literature, highlighting clinical dilemmas, and drawing attention to common misunderstandings, but it does not have the same evidential strength as a systematic review with predefined methods or a controlled study testing outcomes directly in patients. It is therefore best read as a clinical overview rather than a final answer. Even so, the review raises several points that align closely with a broader body of research. Among the most important are that lipedema is not tied to one specific BMI category, that lipedema and obesity are different conditions, that ordinary weight gain can still occur in a person with lipedema, and that the two can coexist in the same body.
In discussions about lipedema, one phrase appears again and again: “Lipedema is not obesity.” That statement is correct, but it is sometimes misunderstood. It does not mean that a person with lipedema cannot also have overweight or obesity. It means that lipedema is a distinct disorder of adipose tissue, with its own tissue characteristics, clinical pattern, and disease mechanisms. Obesity, by contrast, is a broader state of excess body fat associated with metabolic risk, especially when visceral fat accumulates. These are not the same thing, even though they may overlap in one person.
Lipedema is defined by tissue characteristics, not by a single BMI
Lipedema is described in the literature as a chronic, painful disorder of subcutaneous adipose tissue, most often affecting women. It usually presents with symmetrical enlargement of the legs and sometimes the arms, while the feet and hands are relatively spared. The tissue may be painful, bruise easily, feel nodular, and become progressively more fibrotic over time. Because diagnosis is based on tissue pattern and clinical features rather than body weight alone, lipedema can be present across a wide BMI spectrum. Studies and reviews have described lipedema in women with lower, normal, and higher BMI, and even case literature shows that marked weight loss or very low body weight does not necessarily eliminate the disease pattern.
If you want to go deeper, understand the science, and take an active role in your own journey, becoming a paid subscriber to LipedemaScience may be exactly what you need. It is for those who want knowledge, reflection, and a stronger foundation for navigating lipedema with intention. Become a member today.
This point is important because body weight can easily distort the conversation. If a woman has a normal BMI, some assume she cannot have lipedema. If she has a higher BMI, others assume what they are seeing must only be obesity. Neither assumption is reliable. BMI is a rough screening measure based on total mass relative to height. It does not reveal what kind of fat is present, how that fat is distributed, or whether the tissue is structurally altered. That is one reason lipedema is so often misunderstood and misclassified.
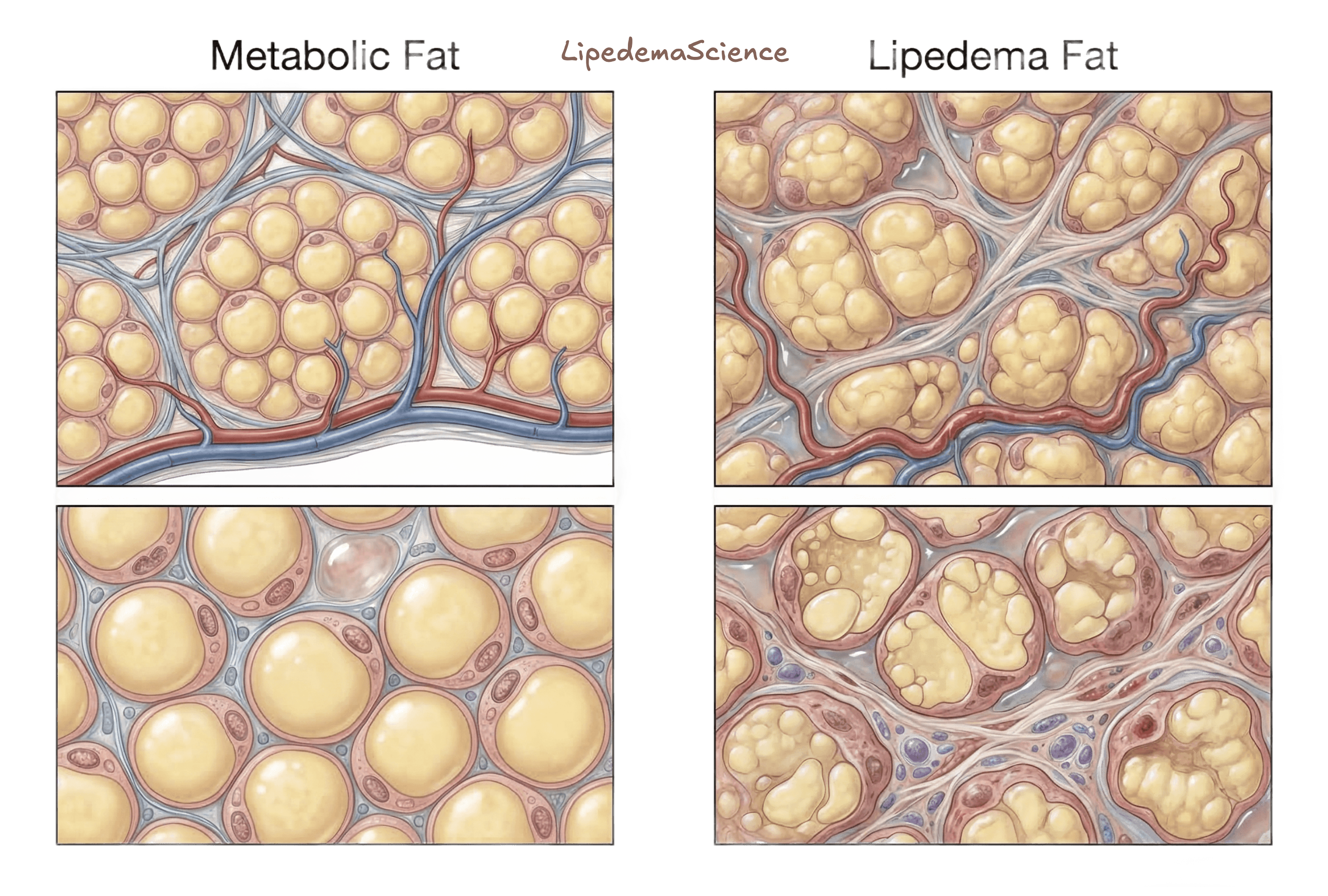
Lipedema fat and metabolic fat are not the same
A helpful way to think about this is to distinguish between metabolic fat and lipedema fat. Metabolic fat is the ordinary adipose tissue that stores and releases energy in response to long term energy balance. It can expand with sustained energy surplus and shrink with sustained energy deficit through the usual processes of lipid storage and mobilization. Its metabolic consequences depend greatly on where it is located. Visceral fat, for example, is more strongly linked to insulin resistance and cardiometabolic risk than lower body subcutaneous fat.
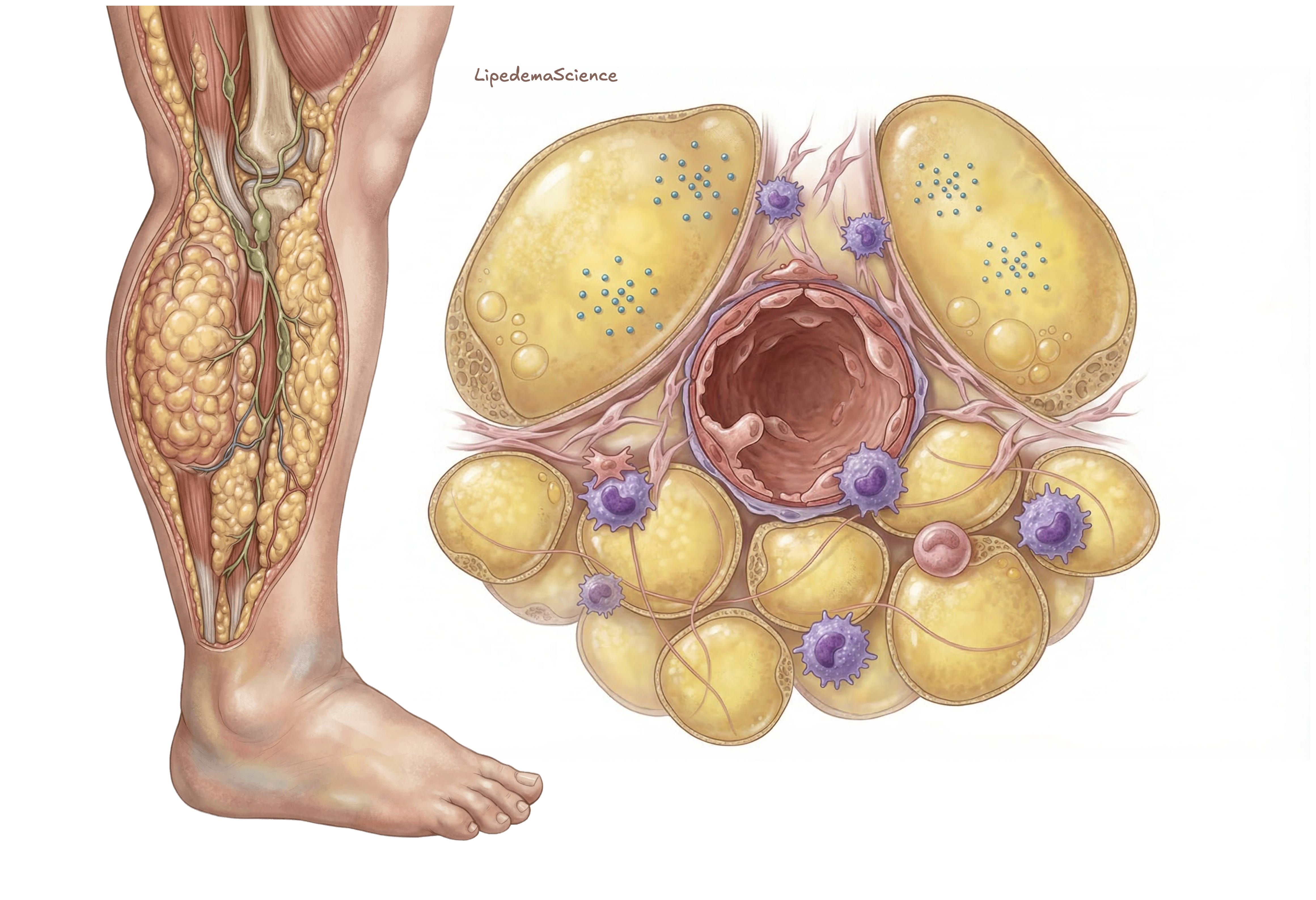
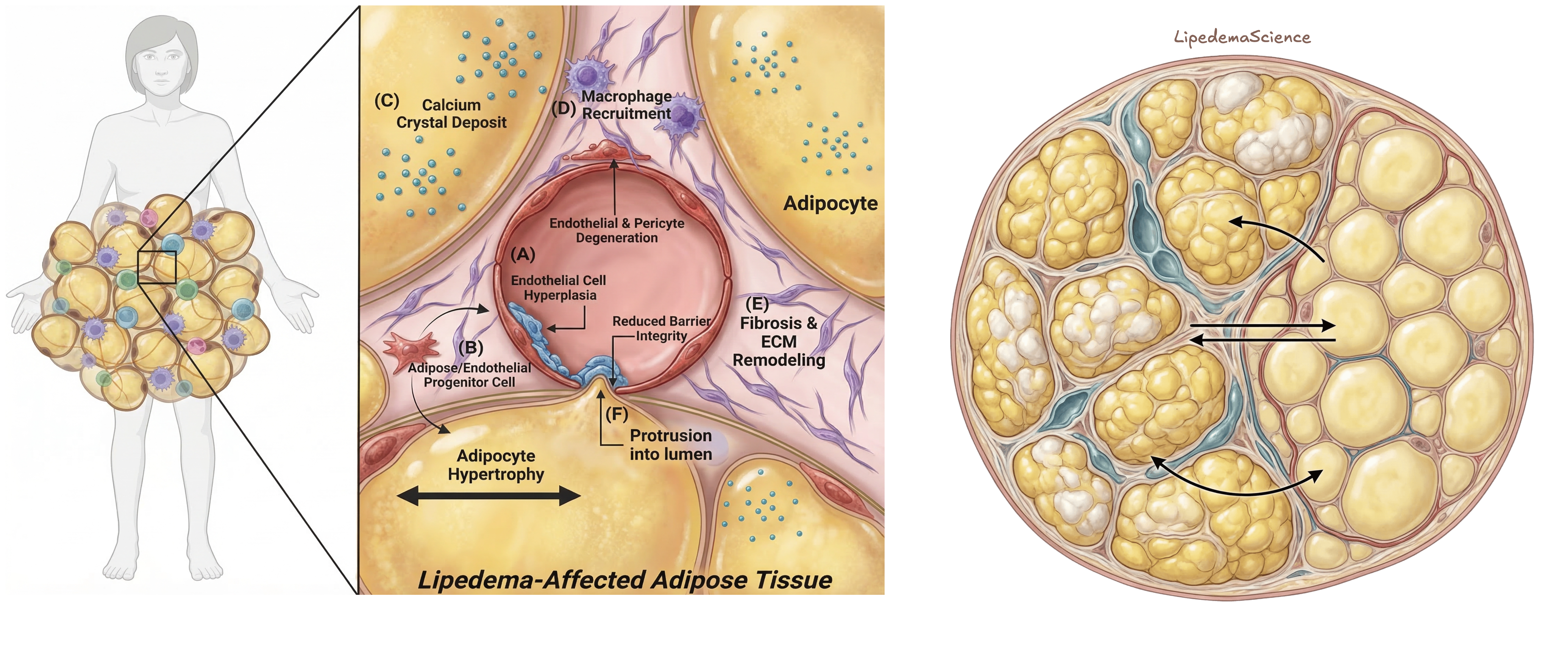
Lipedema fat appears to behave differently. The tissue is not simply a larger amount of ordinary fat. Histologic and mechanistic studies describe adipocyte hypertrophy, increased interstitial fibrosis, altered extracellular matrix, immune cell involvement, and microvascular or lymphatic abnormalities in affected regions. The disease process seems to involve tissue remodeling rather than energy storage alone. In that sense, lipedema fat is biologically active, but it is active in a distinctive and pathologic way.
One important nuance is that lipedema fat is not “dead” fat. A study examining lipid composition and stromal vascular fraction in lipedema tissue found that the lipid composition itself was not dramatically different from control tissue, but the stromal vascular fraction showed altered cytokine signaling and increased mitochondrial respiration. That supports the view that lipedema tissue remains metabolically active, while still being structurally and immunologically abnormal.
Two fat compartments can exist in the same body
This is where the discussion becomes especially important. A person with lipedema does not stop having normal adipose biology simply because they also have lipedema. They still carry ordinary subcutaneous fat, and some may also carry visceral fat. Those fat compartments can still respond to energy surplus and energy deficit in the usual way. This means that a woman with lipedema can gain additional metabolic fat over time, just like anyone else, if energy intake chronically exceeds energy expenditure. When that happens, lipedema and obesity are coexisting in the same body.
This is one of the clearest ways to avoid confusion. Saying that lipedema is not obesity is medically accurate. But saying that lipedema therefore has nothing to do with weight gain at all would go too far. The more precise statement is that lipedema is not defined by obesity, yet a person with lipedema can still gain ordinary metabolic fat and can therefore also meet criteria for overweight or obesity. These realities do not cancel each other out.
Why BMI can be misleading in lipedema
BMI does not distinguish between lipedema tissue, ordinary subcutaneous fat, and visceral fat. A person may therefore fall into an overweight or obesity category on paper for more than one reason. Extra mass from lipedema tissue itself may increase BMI. At the same time, additional metabolic fat may also accumulate, especially if pain, reduced mobility, delayed diagnosis, or emotional strain make weight regulation harder. The result is that BMI can reflect total mass without clarifying the biological sources of that mass.
That matters because lipedema is often mistaken for obesity alone, and obesity is often assumed to explain everything in a body with lipedema. Both errors can lead to poor care. A person may be told simply to lose weight, even when the underlying disease pattern would still remain. On the other hand, discussions within patient communities can become overly rigid, as though any meaningful weight gain must be irrelevant because “lipedema is not obesity.” The literature supports a more nuanced view than either extreme.
What the research suggests about weight loss
The 2024 Diabetes study is especially helpful here. In women with lipedema and obesity, moderate diet induced weight loss of about 9 percent reduced lower body fat volume and improved metabolic function. However, markers associated with inflammation and fibrogenesis in affected adipose tissue remained. In simple terms, some fat was clearly lost, but the deeper tissue pathology did not disappear to the same degree. This helps explain why many women report that they can lose weight, including some fat in the affected areas, while their characteristic proportions and tissue feel remain recognizably lipedemic.
This does not mean weight loss is meaningless. It may reduce total fat mass, improve insulin sensitivity, lower mechanical burden, and support overall health. But it does suggest that weight loss alone does not “cure” lipedema, because the pathological tissue architecture can persist even when the metabolically flexible fat component becomes smaller.
This distinction also fits with lived experience reported by many women. They often describe becoming leaner overall while still seeing the same lower body disproportion, persistent nodularity, or familiar tissue texture. Research cannot yet explain every detail of those experiences, but current findings on fibrosis, adipocyte hypertrophy, tissue remodeling, and stromal signaling make those reports biologically plausible.
Metabolic risk in lipedema is not identical to classic obesity
Another important nuance is that lipedema does not seem to carry the same metabolic profile as classic lifestyle related obesity. In the 2025 Biomedicines study comparing women with lipedema to women with lifestyle induced overweight or obesity, the lipedema group had a more favorable metabolic profile despite high BMI. Impaired glucose metabolism and insulin resistance were less common, and dyslipidemia was also less prevalent. The authors concluded that fat distribution, not just total adiposity, appears to shape metabolic risk.
This does not mean lipedema fat is harmless or that metabolic risk is absent. It means the risk profile may differ from the one most strongly associated with central or visceral adiposity. In other words, a high BMI in lipedema does not automatically imply the same metabolic status as a similar BMI in someone whose fat is distributed differently. That is one reason it is important not to reduce all higher weight bodies to one biological category.
At the same time, a more favorable metabolic profile does not remove the real burden of lipedema. The disease may still involve pain, heaviness, mobility limitations, easy bruising, edema tendency, and significant psychological strain. A person can therefore be relatively protected from some cardiometabolic complications while still being deeply affected in mechanical, vascular, inflammatory, and psychosocial ways.
Why coexistence can make symptoms worse
When obesity coexists with lipedema, the burden on the body can increase. Reviews and observational studies suggest that higher BMI may worsen lymphatic overload, fluid handling, and mobility difficulties. The issue is not that obesity creates lipedema, but that additional body mass may intensify the pressure placed on tissues that are already mechanically and microvascularly vulnerable. In advanced disease, this may contribute to more swelling, reduced function, and progression toward lipo lymphedema in some patients.
This is one reason the coexistence of lipedema and obesity deserves careful language. It is not helpful to frame the issue in a blaming way, and it is equally unhelpful to deny that additional metabolic fat can matter. A person living with both conditions is not simply living in a larger version of the same disease. They may be experiencing two overlapping processes, each of which can affect symptoms, function, and treatment planning.
Why this conversation needs care
This topic can become sensitive very quickly because it touches identity, stigma, body image, and the long history of women with lipedema being dismissed. Many patients have been told for years that their disease was simply obesity. That misclassification has caused real harm. At the same time, some community discussions now swing so far in the opposite direction that any mention of weight gain or obesity feels invalidating. The research supports a middle position that is both more accurate and more humane. Lipedema is a distinct disease. Obesity is a different condition. They can overlap. Weight change can still occur. And none of this should be used to judge the person living in that body.
A more biologically grounded way to say it is this: people with lipedema may carry both disease specific lipedema tissue and ordinary metabolic fat. These compartments do not behave identically. Weight loss may reduce the metabolically flexible component while leaving the disease specific tissue architecture relatively unchanged. Weight gain may increase the ordinary fat compartment even though the underlying lipedema remains a separate process. That framework is consistent with both the literature and the experiences many women describe.
Moving toward a more accurate understanding
The most constructive conclusion is not that weight is irrelevant in lipedema, and not that lipedema is simply another name for obesity. The better conclusion is that these are different but potentially overlapping realities. Lipedema is a disorder of adipose tissue and connective tissue with a recognizable clinical pattern and distinct tissue biology. Obesity is a broader state of excess adiposity, often with metabolic implications that depend heavily on fat distribution. A person may have one, the other, or both. Recognizing that complexity helps clinicians assess patients more accurately, helps patients make sense of their bodies with less self blame, and helps public discussion move away from simplistic categories and toward clearer biological understanding.
Lipedema and obesity: A narrative review and treatment protocol (DOI: 10.1016/j.jpra.2026.01.004)
Adipose tissue biology and effect of weight loss in women with lipedema (DOI: 10.2337/db24-0890)
Metabolic Alterations in Women with Lipedema Compared to Women with Lifestyle-Induced Overweight/Obesity (DOI: 10.3390/biomedicines13040867)
A Distinct Cytokine Profile and Stromal Vascular Fraction Metabolic Status without Significant Changes in the Lipid Composition Characterizes Lipedema (DOI: 10.3390/ijms22073313)
Lipedema stage affects adipocyte hypertrophy, subcutaneous adipose tissue inflammation and interstitial fibrosis (DOI: 10.3389/fimmu.2023.1223264)
Lipedema: A Disease Triggered by M2 Polarized Macrophages? (DOI: 10.3390/biomedicines13030561)
Lipedema and adipose tissue: current understanding, controversies, and future directions (DOI: 10.3389/fcell.2025.1691161)
Key signaling networks are dysregulated in patients with the adipose tissue disorder, lipedema (DOI: 10.1038/s41366-021-01002-1)
Lipedema is not obesity – A call for clinical clarity (DOI: 10.1016/j.jacl.2025.11.004)
Lipedema: Clinical Features, Diagnosis, and Management (DOI: 10.1055/a-2530-5875)
Lipoedema is not lymphoedema: A review of current literature (DOI: 10.1111/iwj.12949)
Lipedema: A Relatively Common Disease with Extremely Common Misconceptions (DOI: 10.1097/GOX.0000000000001043)
Hedonic hunger and eating behavior after low-carbohydrate versus low-fat diets in females with lipedema and obesity (DOI: 10.3389/fnut.2025.1716592)
Lipedema Research—Quo Vadis? (DOI: 10.3390/jpm13010098)
Lipedema: Insights into Morphology, Pathophysiology, and Challenges (DOI: 10.3390/biomedicines10123081)
A Young Woman with Excessive Fat in Lower Extremities Develops Disordered Eating and Is Subsequently Diagnosed with Anorexia Nervosa, Lipedema, and Hypermobile Ehlers-Danlos Syndrome (DOI: 10.12659/AJCR.930840)
Lipedema: friend and foe (DOI: 10.1515/hmbci-2017-0076)
Lipedema and the Evolution to Lymphedema With the Progression of Obesity (DOI: 10.7759/cureus.11854)
Lymphoscintigraphic alterations in lower limbs in women with lipedema in comparison to women with overweight/obesity (DOI: 10.3389/fphys.2023.1099555)