
Why Sugar Hurt My Lipedema Tissue Before Surgery
A personal reflection on acute swelling, pain, and why the reaction changed after liposuction.

This article starts with a personal observation. It is not a clinical conclusion. It is not proof. It is my own reflection as someone who has lived with lipedema, worked with science, and spent years trying to understand why my body reacted the way it did.
Before my lipedema surgeries, refined sugar was one of the clearest and most immediate symptom triggers I had. I could eat many foods without dramatic reactions, but white, refined sugar was different. It could trigger a very specific kind of pain and swelling in my legs. The pain felt deep, aching and inflammatory, almost like a toothache inside the tissue. The swelling could come quickly, and at its worst, my legs felt as if they changed size within a short time.
What made this especially interesting to me was that the reaction was not simply “carbohydrates are bad”. I did not experience white flour in exactly the same way. The strongest reaction was linked to refined sugar and rapid sugar exposure. Before surgery, it felt as if the lipedema tissue itself was reacting acutely.
After my liposuction surgeries, this changed. I am not saying that diet no longer matters, or that sugar is suddenly biologically neutral. But the dramatic acute reaction I used to experience in the lipedema tissue is no longer the same. The intense swelling and pain response that I associated with refined sugar largely disappeared after a substantial amount of diseased fat tissue had been removed.
That observation has made me think about lipedema in a very concrete way. What if the reaction was not only about sugar itself, but about sugar entering a tissue environment that was already inflamed, fluid sensitive, microvascularly fragile and pain sensitized?
This is where my personal experience meets the mechanistic theory.
Lipedema tissue is increasingly described as more than enlarged fat tissue. Studies have reported adipocyte hypertrophy, immune cell activity, microvascular changes, increased capillary fragility, extracellular matrix remodeling, fibrosis, pain sensitivity and signs of altered lymphatic or fluid handling. The exact biology is still debated, and not every study finds the same inflammatory pattern, but the overall picture suggests that lipedema tissue can be biologically reactive.
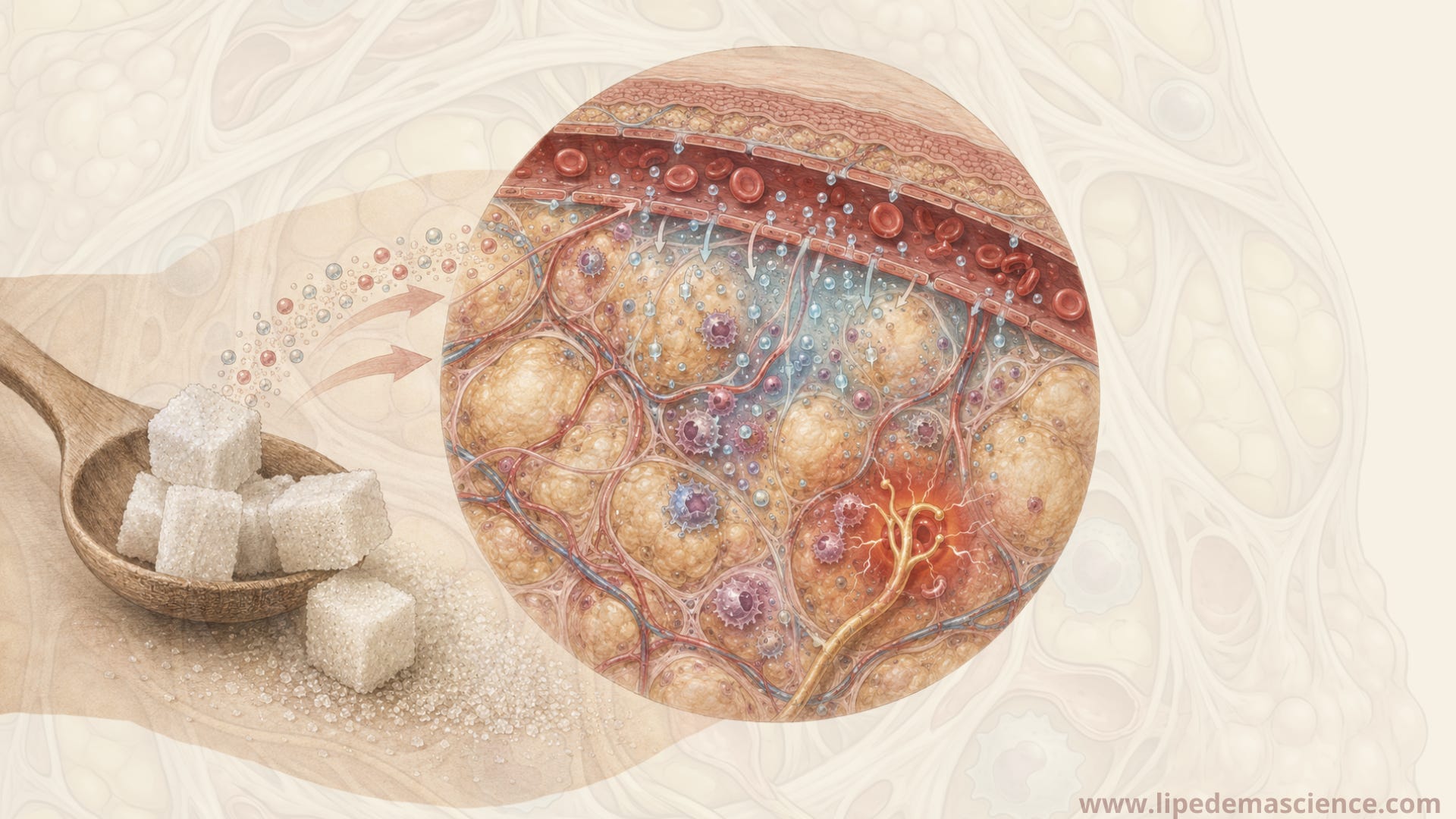
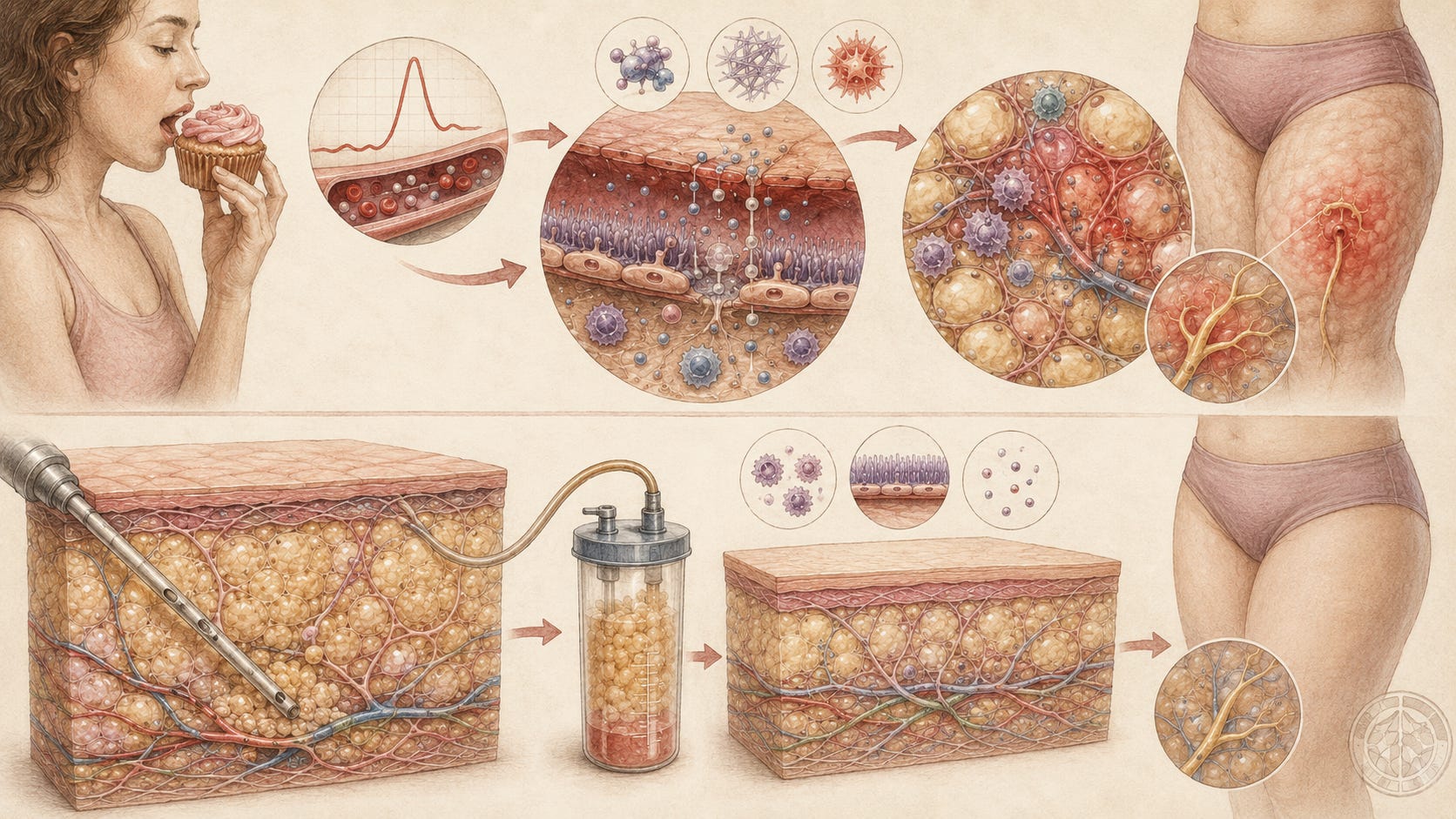
If a tissue is already close to a threshold, it may not take much to push it into a symptomatic state. A high sugar load can create a rapid postprandial response. Blood glucose rises, insulin rises, oxidative stress can increase, inflammatory signaling can be activated, and the vascular endothelium can become more permeable. In general physiology, acute hyperglycemia has been linked to endothelial dysfunction and damage to the endothelial glycocalyx, the protective layer that helps regulate vascular permeability. Insulin can also promote sodium retention, and sodium draws water with it.
In normal tissue, this may not be felt as pain. But in lipedema tissue, the situation may be different. If the microvasculature is already fragile, if lymphatic drainage is already less efficient, if the extracellular matrix already binds fluid, and if the nerves are already sensitized, then a postprandial sugar response could theoretically become a local swelling and pain event.
In that model, sugar is not “creating lipedema”. It is exposing the vulnerability of the tissue.
The acute reaction could be understood as a kind of perfect storm. A rapid glucose and insulin response may increase sodium and water retention. Endothelial stress may increase leakage from the capillaries. Low grade inflammatory signaling may lower the pain threshold. Fluid moves into a tissue that already struggles with fluid handling. The tissue pressure rises. Pain nerves that are already sensitized respond more strongly.

This could explain why the pain felt so deep and immediate. It may not have been ordinary “diet discomfort”. It may have been a local tissue reaction in a pathological fat compartment.
This is also why the change after liposuction is so interesting. Liposuction for lipedema does not only change body shape. It removes a large volume of the pathological fat tissue that may be driving pain, fluid retention and inflammatory signaling. In several surgical studies, patients report long lasting reductions in pain, tenderness, bruising, edema and mobility limitations after liposuction. The mechanism is still not fully understood, but the simplest explanation is that removing diseased, reactive tissue reduces the biological substrate that can generate symptoms.
In my case, this is exactly what it felt like. The same body, the same person, but with much less reactive lipedema tissue. After surgery, there was simply less tissue available to swell, retain fluid, produce inflammatory signals and amplify pain.
I think this is a more plausible explanation than the idea that surgery works mainly by “cutting nerves”. That theory is sometimes mentioned informally, but it is not well established in the lipedema literature. Modern lipedema liposuction techniques are designed to be tissue sparing, especially toward lymphatic structures, vessels and nerves. Temporary sensory changes can happen after surgery, but that is not the same as saying that long term pain relief is caused by intentional denervation.

To me, the more convincing explanation is substrate reduction. Less pathological tissue means less inflammatory capacity, less fluid binding capacity, less mechanical pressure and less nociceptive input. If sugar previously triggered an acute reaction in that tissue, then removing much of the tissue could logically reduce or stop the reaction.
There is also some dietary research that makes this question even more relevant. Small studies on low carbohydrate or ketogenic diets in lipedema suggest that pain may improve independently of weight loss, and that pain can return when carbohydrates are reintroduced. These studies are still small and should not be overinterpreted, but they support the idea that carbohydrate metabolism may influence lipedema pain in ways that are not only about body weight.
Still, there are important limitations. To my knowledge, no study has directly measured acute sugar induced swelling in lipedema tissue before and after a glucose or sugar challenge. No study has taken patients like me, measured tissue water, tissue sodium, inflammatory markers and pain response after sugar intake, and then repeated the same measurements after liposuction. That is the study I wish existed.
So this remains a theory. A biologically plausible theory, but still a theory.
My personal interpretation is this: before surgery, refined sugar triggered a rapid inflammatory and fluid related response in my lipedema tissue. The tissue was already vulnerable. It was probably more prone to fluid retention, vascular leakage, pressure and pain signaling. After surgery, much of that reactive tissue was removed, and the acute sugar reaction largely disappeared.
That does not mean everyone with lipedema will experience the same thing. Lipedema is not identical from person to person. Some people may react strongly to sugar. Others may not. Some may respond to low carbohydrate diets. Others may do better with a different nutritional strategy. Surgery may reduce symptoms dramatically for some, while others still need compression, movement, lymphatic support and careful symptom management.
But I do think these personal observations matter. They can help generate better research questions. Why do some patients report acute swelling and pain after sugar? Is it linked to insulin, sodium, endothelial permeability, inflammation, lymphatic load, nerve sensitization or all of these at once? Does liposuction change this response because it removes the pathological tissue substrate? Could tissue sodium MRI, water imaging or postprandial inflammatory markers help us understand this better?
For me, the experience changed how I think about lipedema. It made the disease feel less mysterious and more biological. The pain was not imagined. The swelling was not random. The sugar reaction was not a moral failure or a lack of discipline. It felt like a measurable tissue response that science has simply not studied properly yet.
And that is where I think we need to go next. Not toward simplistic diet rules, but toward mechanisms. Not toward blaming patients for what they eat, but toward understanding why some lipedema tissue reacts so strongly in the first place.
Have you experienced something similar? Did sugar or other high-carbohydrate foods trigger pain, heaviness, swelling, or tenderness in your lipedema tissue before surgery? And if you have undergone liposuction, did those reactions change afterward?
I would love to hear about your experience in the comments. Personal observations are not scientific proof, but they can help identify patterns and generate important research questions.