
When Your Fat Tissue Starts Sending Inflammatory Signals
I first learned about cytokines in the lab while studying inflammatory responses. Then I started recognizing the same language in my own body.

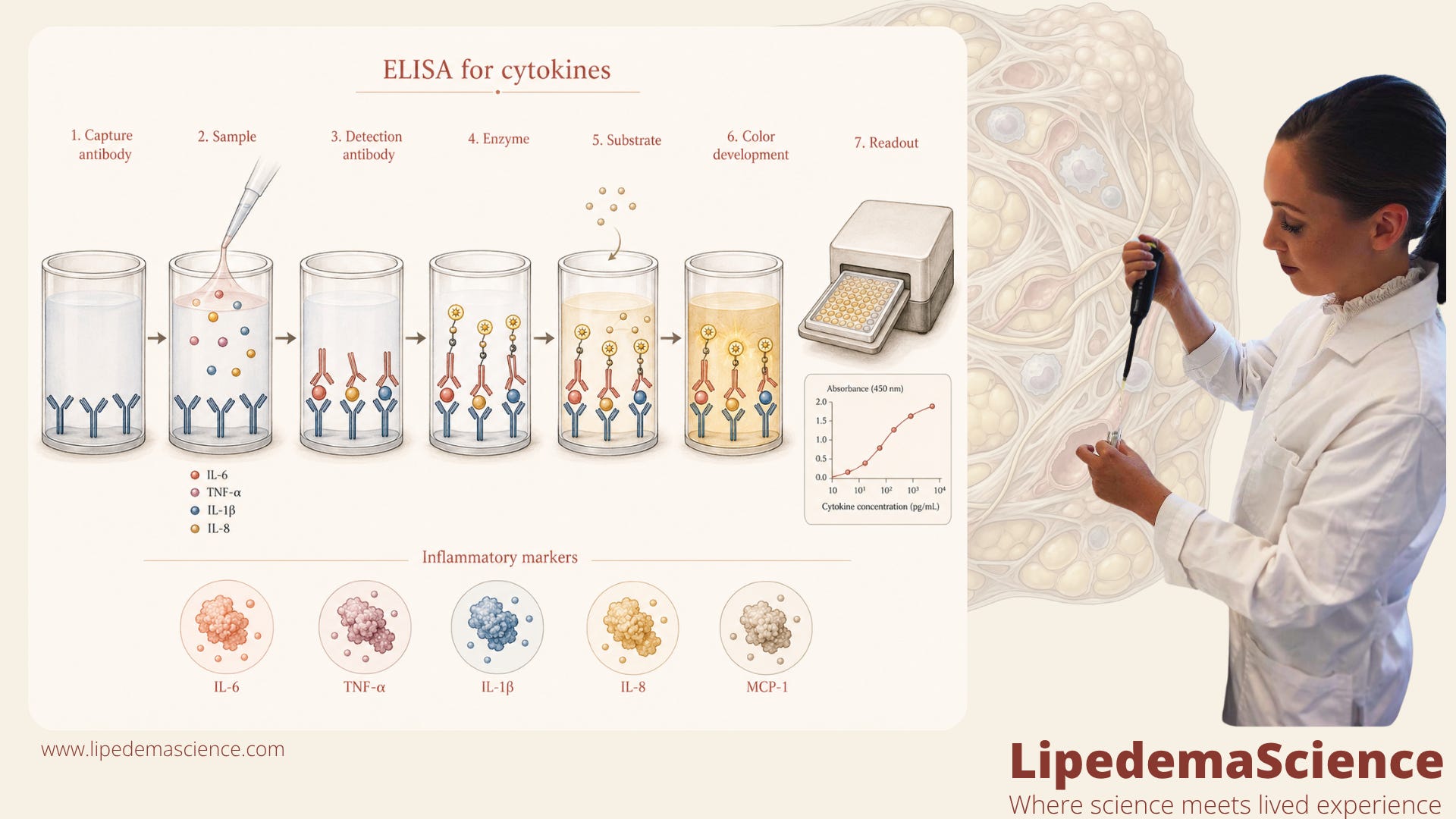
In 2020, while I was working on my master’s thesis, I spent a lot of time in the lab studying inflammatory responses. I worked with a method called ELISA, which is used to measure specific proteins in biological samples. In my case, I was looking at inflammatory signals related to pea peptides, using models involving IL 8 and IL 1 beta. That was when cytokines stopped being abstract textbook words for me. They became a language.
I began to understand that inflammation is not just one thing. It is not simply “being inflamed” or “not being inflamed.” It is a whole communication system inside the body. Cytokines are some of the small signaling molecules that help immune cells, blood vessel cells, fat cells and other tissues talk to each other. Sometimes they help the body repair. Sometimes they help defend. But when the signaling becomes too loud, too persistent, or poorly regulated, that same language can start to feel like pain, swelling, heat, tenderness and fatigue. And for me, that suddenly made something personal click.
Long before I understood cytokines, I had noticed something strange in my own body. Already before 2016, I could feel a reaction after eating white refined sugar. Not glucose in a laboratory sense. Not complex carbohydrates in general. But white refined sugar. Within minutes, I could feel a kind of inflammatory response in my lipedema tissue. My legs could feel heavier, tighter, more swollen, almost as if something had been switched on inside the tissue.
At the time, I did not have the language for it. Later, when I started learning about IL 8, IL 1 beta and the wider cytokine network, I began to wonder whether what I was feeling was not random at all. Maybe it was not “just sensitivity.” Maybe it was not “just in my head.” Maybe my tissue was responding through the same kind of inflammatory signaling systems I was measuring in the lab.
That is why I want you to understand cytokines. Not because everyone with lipedema needs to become an immunologist. Not because cytokines explain everything about lipedema. They do not. But because cytokines may help us understand why lipedema can feel so reactive. Why symptoms can flare after stress, poor sleep, hormonal shifts, certain foods, infections, overexertion or long periods of standing. Why the tissue can feel alive with signals. Why pain and swelling can change so quickly, even when body weight has not changed at all.
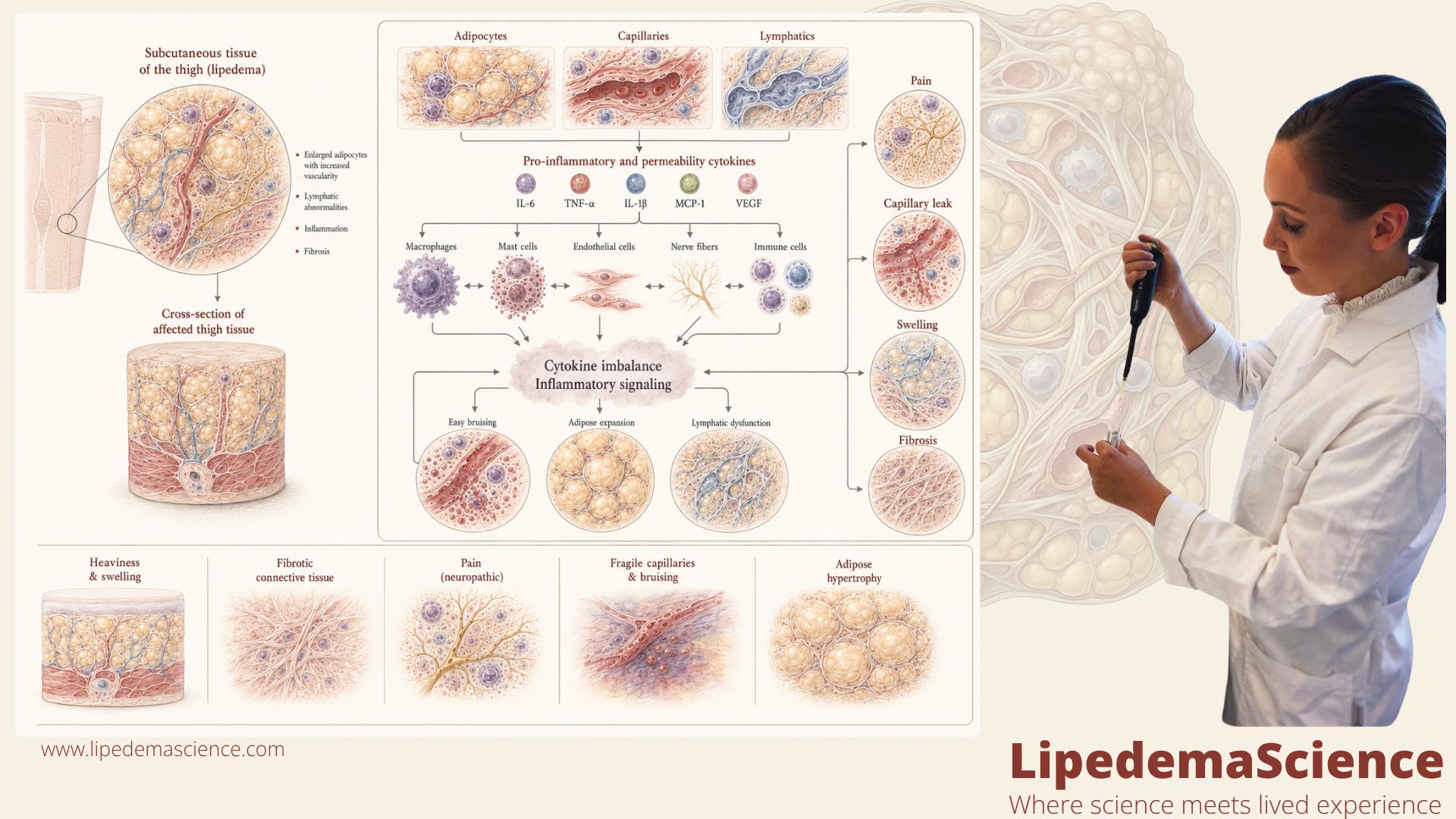
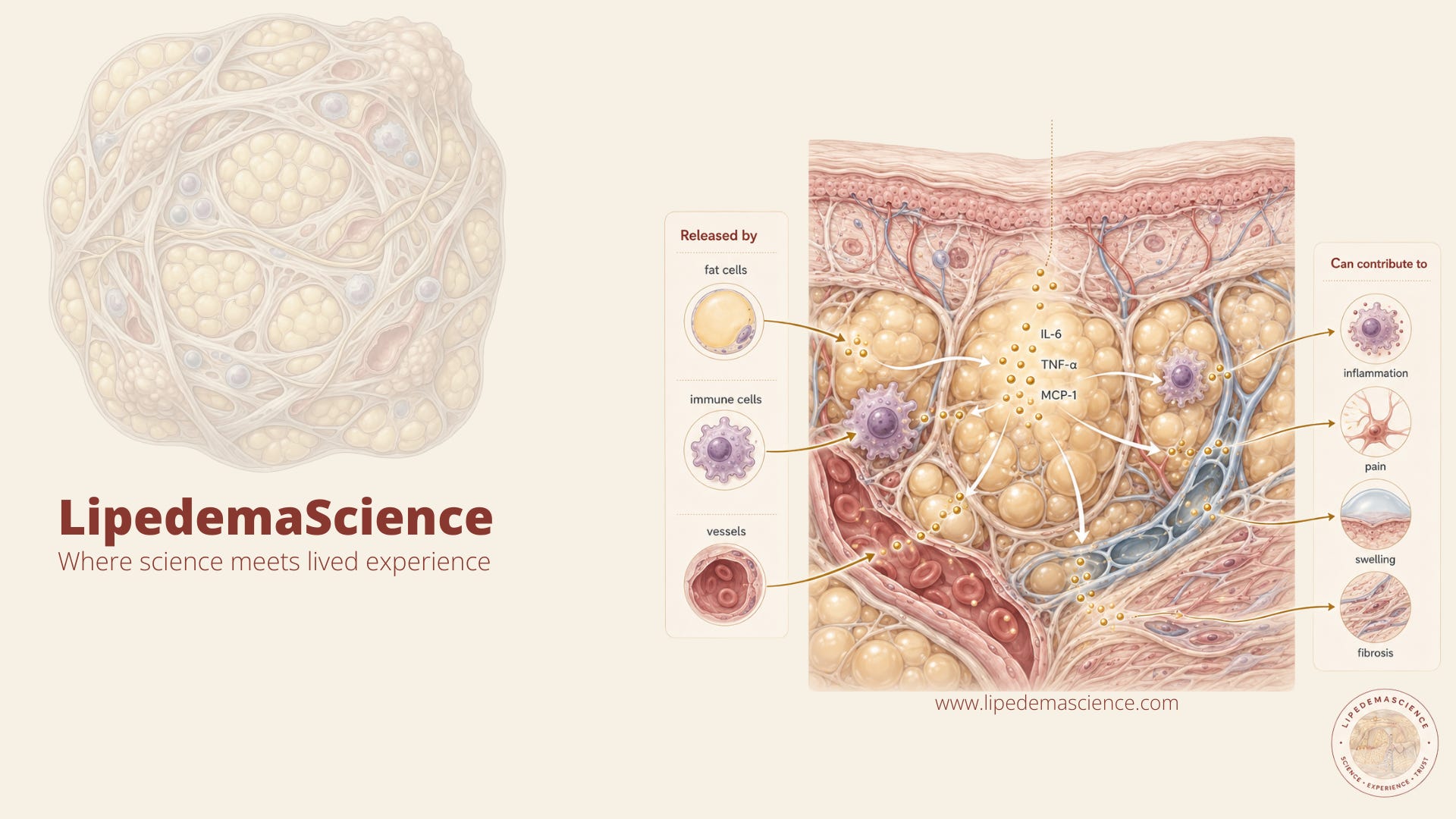
Lipedema tissue is not passive fat. It is an active biological environment made up of fat cells, immune cells, blood vessel cells, connective tissue cells and nerve endings. These cells are constantly communicating. In lipedema, research suggests that parts of this communication system may become unbalanced, with inflammatory and tissue remodeling signals contributing to pain, swelling, vascular leakiness, fibrosis and changes in fat tissue behavior.
This is where cytokines matter. They are not just tiny molecules with complicated names. They may be part of the reason lipedema tissue feels tender, swollen, heavy, reactive and difficult to calm down.
If we want to understand lipedema as a real biological disease, we need to understand the signals inside the tissue. The ones that may help explain pain. Swelling. Flares. Tenderness. Fibrosis. And the strange feeling that your tissue is reacting long before anyone else can see what is happening.
Become a member of LipedemaScience today.
The founder of LipedemaScience was diagnosed with lipedema at a Norwegian hospital in 2012. She has worked in the lab and with science for many years. Her passion is to share knowledge about lipedema, and that is why she has built this unique space and community.
Why cytokines matter in lipedema
To understand why cytokines matter in lipedema, we first have to move away from the idea that fat tissue is just storage.
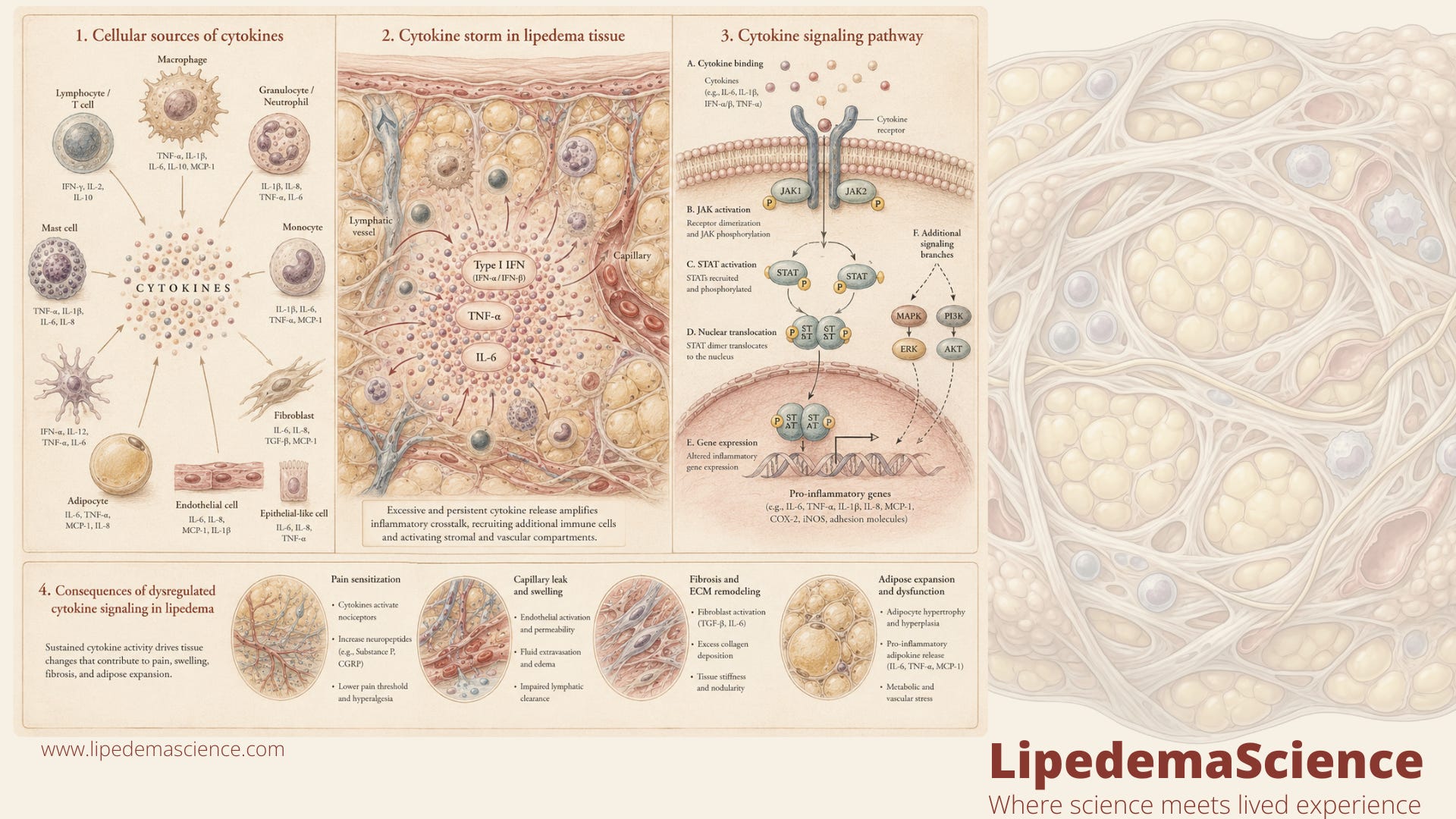
Fat tissue is not a passive container for excess energy. It is an active endocrine and immune organ. It contains fat cells, immune cells, blood vessel cells, connective tissue cells, stem like precursor cells, nerve endings and lymphatic structures. All of these cells communicate. They send signals, receive signals, react to stress, respond to injury, and change their behavior depending on the biochemical environment around them.
Cytokines are part of that communication system. They are small signaling proteins that help cells coordinate immune activity, inflammation, tissue repair and metabolic responses. In a healthy situation, this signaling is tightly regulated. A signal rises when it is needed, helps organize a response, and then quiets down again when the job is done.
But when cytokine signaling becomes chronic, exaggerated or poorly resolved, the body can get stuck in a state where the tissue behaves as if something still needs to be repaired, defended or remodeled.
This is where lipedema becomes interesting. Lipedema tissue does not behave like ordinary fat. People with lipedema often describe tissue that feels painful, heavy, swollen, bruised, inflamed, pressure sensitive and strangely reactive. Symptoms can worsen after hormonal shifts, stress, poor sleep, heat, long standing, certain foods or intense physical load. The frustrating part is that these changes can happen quickly, sometimes long before there is any visible change in body size.
That makes more sense when we stop thinking only in terms of fat volume and start thinking in terms of tissue signaling.
A flare is not necessarily “more fat.” A flare may be the tissue environment changing. Blood vessels may become more permeable. Fluid may move into the tissue. Immune cells may become more active. Nerves may become more sensitive. The extracellular matrix may become stiffer. The whole local environment may shift toward pain, pressure and swelling.
Cytokines are not the whole explanation, but they are one of the biological languages through which this may happen.

The tissue is not silent
One of the most important things to understand is that lipedema tissue appears to be biologically active.
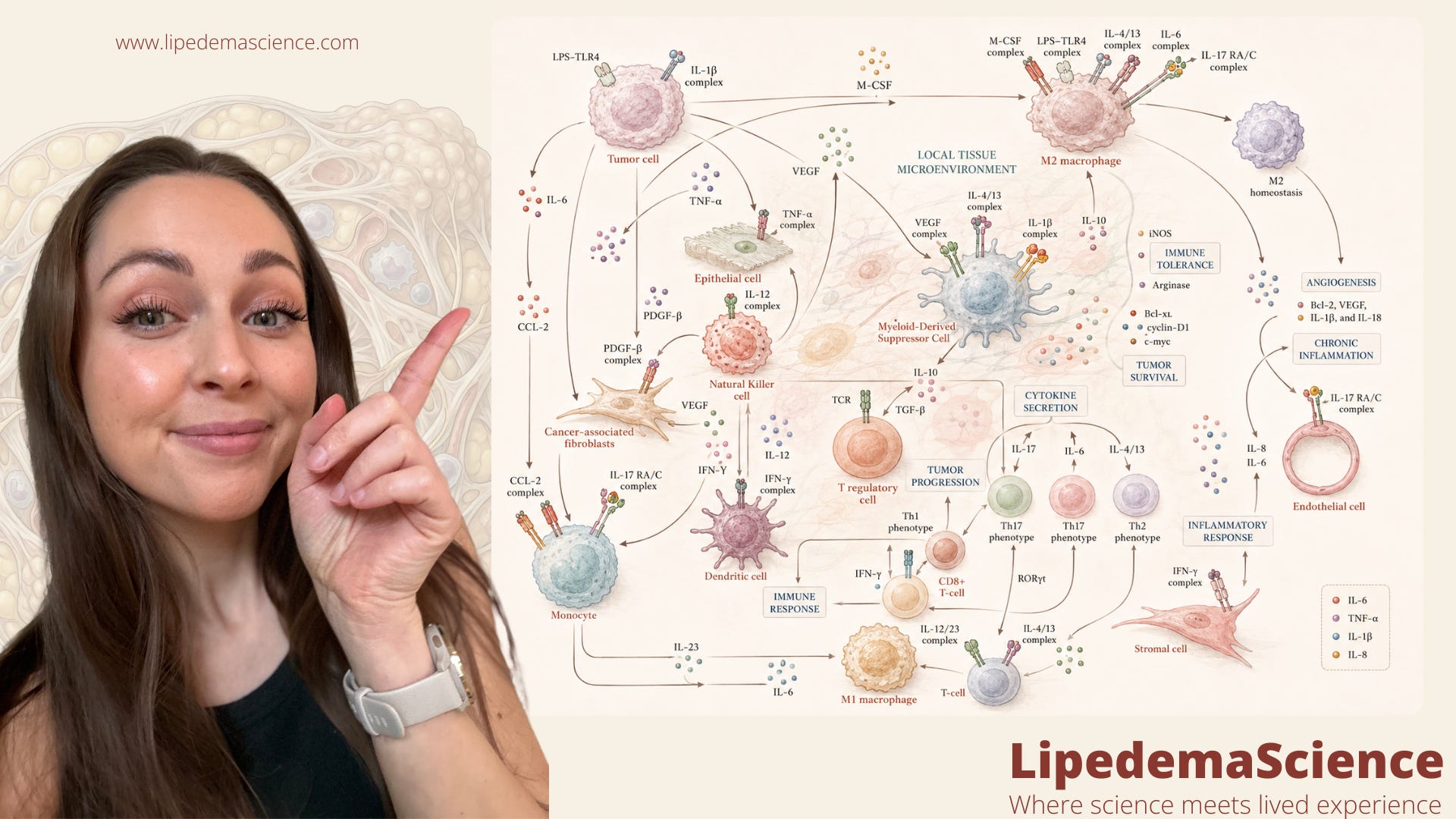
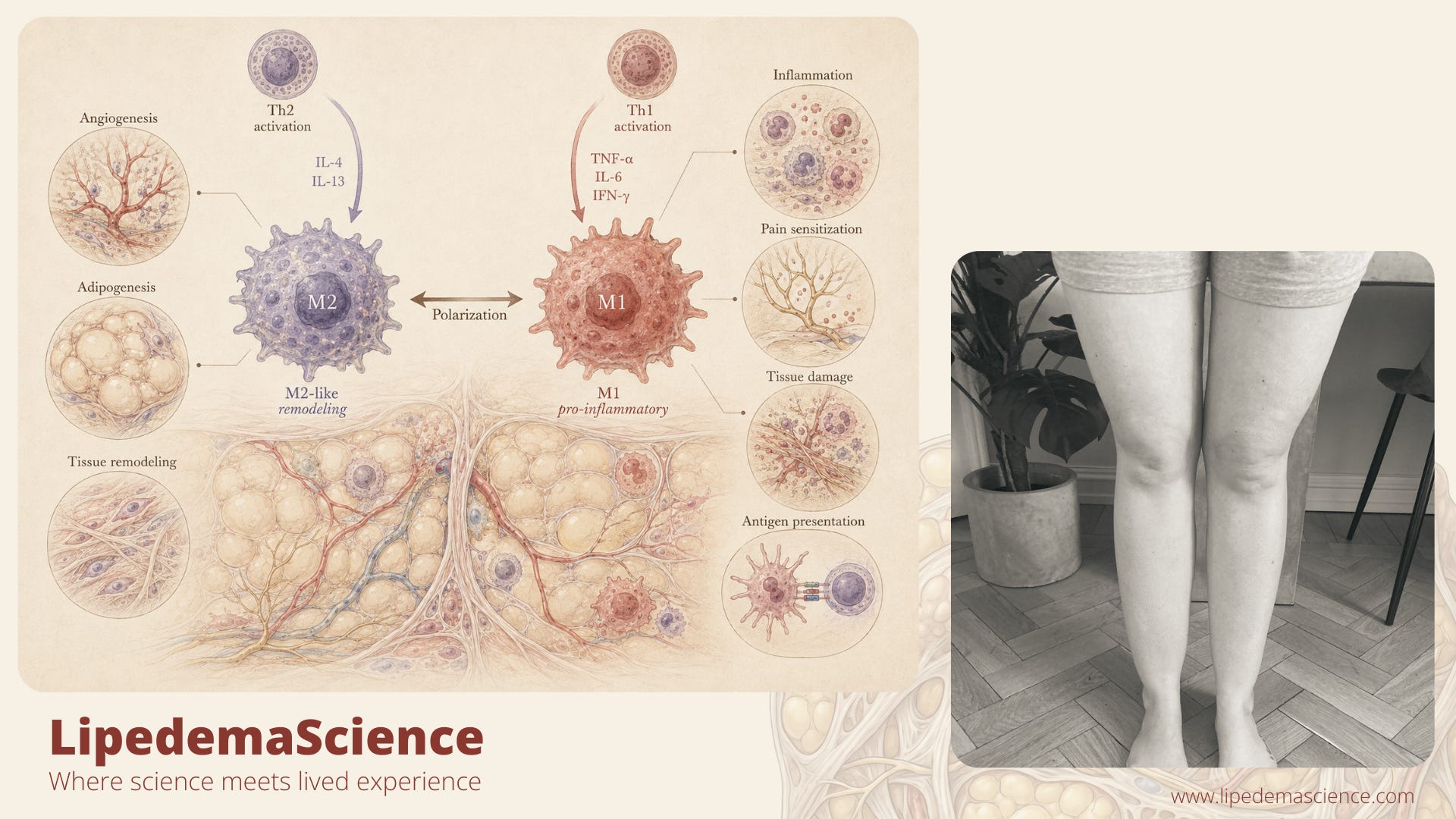
Research has found differences in inflammatory signaling, macrophage behavior, vascular function, adipocyte biology, fibrosis and gene expression in lipedema tissue. Some studies point toward macrophages, especially M2 like macrophage populations, as important players in the tissue environment. Others show changes related to inflammation, pain, extracellular matrix remodeling, blood vessel permeability and adipogenesis.
This matters because macrophages are not just “immune cells.” They are tissue organizers. They help decide whether a tissue environment moves toward repair, remodeling, fibrosis, inflammation or fat cell development.
If macrophages and other immune cells release cytokines in a pattern that promotes tissue remodeling, vascular leakiness, nerve sensitivity or adipocyte growth, then lipedema symptoms become easier to understand. The pain is not random. The swelling is not imaginary. The heaviness is not simply a failure of discipline. It may reflect a tissue environment where inflammatory and repair signals are not returning fully to baseline.
This is also why the word “inflammation” can be both useful and misleading.
Lipedema is not necessarily inflammation in the simple sense of a hot, infected wound. It may be more subtle than that. It may involve low grade, chronic, local immune signaling inside adipose tissue. Enough to affect nerves, vessels, connective tissue and fat cell behavior, but not always enough to show up clearly in standard blood tests.
That is why many people can feel inflamed even when their routine blood work looks normal.
The cytokines you do not need to memorize, but should understand
You do not need to remember every cytokine name. But it helps to understand the pattern.
IL 6 is often discussed in relation to inflammation, metabolism, stress responses and pain sensitivity. TNF alpha is another inflammatory cytokine that can influence insulin signaling, vascular function and tissue inflammation. IL 1 beta is a powerful inflammatory messenger involved in immune activation and pain related pathways. IL 8 is strongly connected to immune cell recruitment and inflammatory signaling. VEGF is not a cytokine in the narrowest sense, but it is an important signaling molecule because it can increase blood vessel permeability and is often discussed in relation to swelling, vascular changes and tissue remodeling.
Then there is MIF, macrophage migration inhibitory factor, which has also been studied in lipedema. MIF is interesting because it can help sustain inflammatory activity and influence immune cell behavior. If a tissue environment keeps producing signals that maintain immune activation, it becomes easier to imagine why symptoms may keep returning even when someone is doing “everything right.”
The important point is not one single molecule.
The important point is the pattern.
Lipedema research increasingly suggests that the tissue environment may involve an altered conversation between fat cells, immune cells, blood vessels and connective tissue. Cytokines are part of that conversation. When the conversation becomes unbalanced, symptoms may become louder.
Why this can feel like pain, swelling and pressure
So what does this mean inside the body?
Imagine a local area of lipedema tissue where immune cells are active and cytokine signaling increases. Some signals may make small blood vessels more permeable. That means more fluid can move out of the bloodstream and into the surrounding tissue. When fluid accumulates, pressure rises. The tissue can feel tight, heavy and swollen.
Other signals may make sensory nerves more reactive. This means that pressure that should feel neutral can become painful. A light touch, compression garment, massage, sitting position or even the pressure of clothing can feel disproportionately uncomfortable.
Over time, repeated inflammatory and repair signaling may also contribute to fibrosis. Fibrosis means the tissue becomes stiffer and more structurally altered. This can create the rope like, nodular or hardened areas many people with lipedema recognize. Once fibrosis develops, fluid movement may become harder, tissue pressure may increase, and pain may become more persistent.
This is why cytokines matter. They help explain how lipedema can be painful without looking dramatic from the outside. They help explain how swelling can fluctuate. They help explain why the tissue can feel inflamed even when other people cannot see what is happening. And for many of us, that explanation is deeply validating.
Because when your legs suddenly feel heavier after a trigger, when your tissue becomes more painful after poor sleep, when refined sugar seems to switch something on, when stress makes your body feel swollen and bruised, it can be easy to doubt yourself. But biology is full of signals that move faster than visible structural change. Your body can react long before anyone else can see it.
If you want to support my work, I would love to hear your thoughts in the comments, and I would be so grateful if you shared it with someone with lipedema.
A Distinct Cytokine Profile and Stromal Vascular Fraction Metabolic Status without Significant Changes in the Lipid Composition Characterizes Lipedema (DOI: 10.3390/ijms22073313)
Changes in Cytokines and Fibrotic Growth Factors after Low-Carbohydrate or Low-Fat Low-Energy Diets in Females with Lipedema (DOI: 10.1016/j.cdnut.2025.104571)
Lipedema: Insights into Morphology, Pathophysiology, and Challenges (DOI: 10.3390/biomedicines10123081)
Is subcutaneous adipose tissue expansion in people living with lipedema healthier and reflected by circulating parameters? (DOI: 10.3389/fendo.2022.1000094)
Exploring the Anti-Inflammatory Potential of a Mediterranean-Style Ketogenic Diet in Women with Lipedema (DOI: 10.3390/nu17183014)
Involvement of the Macrophage Migration Inhibitory Factor (MIF) in Lipedema (DOI: 10.3390/metabo13101105)
Lipedema: A Disease Triggered by M2 Polarized Macrophages? (DOI: 10.3390/biomedicines13030561)
Lipedema stage affects adipocyte hypertrophy, subcutaneous adipose tissue inflammation and interstitial fibrosis (DOI: 10.3389/fimmu.2023.1223264)
Transcriptomics of Subcutaneous Tissue of Lipedema Identified Differentially Expressed Genes Involved in Adipogenesis, Inflammation, and Pain (DOI: 10.1097/GOX.0000000000006288)
Lipedema: exploring pathophysiology and treatment strategies – state of the art (DOI: doi.org/10.1590/1677-5449.202400252)
Metabolic conditions of chronic inflammatory diseases (DOI: 10.3389/fimmu.2022.1123676)
Pathophysiological dilemmas of lipedema (DOI: 10.1016/j.mehy.2014.08.011)
Lipedema: The Use of Cultured Adipocytes for Identification of Diagnostic Markers (DOI: 10.1097/PRS.0000000000010392)
Current Mechanistic Understandings of Lymphedema and Lipedema: Tales of Fluid, Fat, and Fibrosis (DOI: 10.3390/ijms23126621)
Indications of Peripheral Pain, Dermal Hypersensitivity, and Neurogenic Inflammation in Patients with Lipedema (DOI: 10.3390/ijms231810313)
Endothelial cell alterations in capillaries of adipose tissue from patients affected by lipedema (DOI: 10.1002/oby.24244)
Multi-Level Analysis of Adipose Tissue Reveals the Relevance of Perivascular Subpopulations and an Increased Endothelial Permeability in Early-Stage Lipedema (DOI: 10.3390/biomedicines10051163)
Identification of Specific microRNAs in Adipose Tissue Affected by Lipedema (DOI: 10.3390/cimb46110710)
Therapeutic Applications of Ketogenic Diets in Lipedema: A Narrative Review of Current Evidence (DOI: 14:49 10.1007/s13679-025-00642-y)
Increase in Leptin and PPAR-γ Gene Expression in Lipedema Adipocytes Differentiated in vitro from Adipose-Derived Stem Cells (DOI: 10.3390/cells9020430)
A distinct M2 macrophage infiltrate and transcriptomic profile decisively influence adipocyte differentiation in lipedema (DOI: 10.3389/fimmu.2022.1004609)