
When IVF, Lipedema, and Hormones Collide
A personal reflection on a new study, artificial menopause, and not recognizing my own body.

I am in the middle of IVF.
And for the first time in my life, I feel like I truly do not recognize my own body.
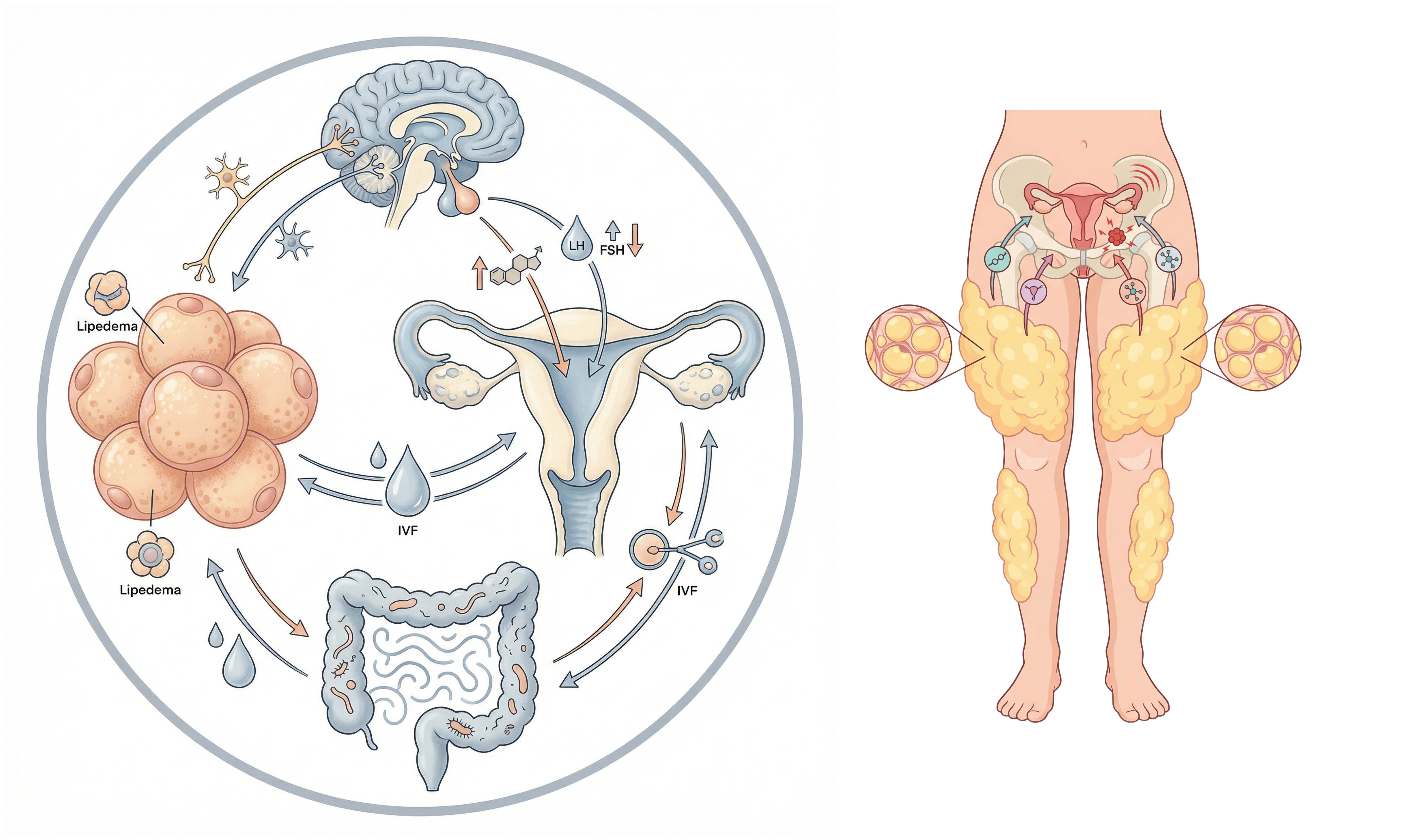
Two weeks ago, I received a depot injection to downregulate my pituitary before stimulation. In practical terms, it means my body has been pushed into a temporary, pharmacological menopause. LH and FSH are suppressed. Estrogen drops dramatically. Everything shifts at once.
Since then, I’ve been retaining so much fluid it feels like the period right after my lipedema surgeries.
My fingers feel tight. My face feels puffy. My abdomen feels swollen and pressurized. My legs feel heavy in a way that is familiar but amplified. I look in the mirror and see a body that feels foreign.
I have been told it will pass.
But living inside it is something else..
And while all of this has been unfolding, I have been reading a new scoping review on lipedema and its interrelationship with endometriosis and other gynecologic diseases.
The more I learn about the hormonal underpinnings of lipedema, the more I wonder whether my ovaries have always been part of the story.
Not broken. Not defective.
But part of a larger endocrine pattern.
IVF has shown me that my body does not respond like everyone else’s
One of the most confronting parts of fertility treatment is comparison.
You sit in waiting rooms with women who respond quickly. You read forums where stimulation leads to predictable follicle growth. You see hormone curves that behave as textbooks suggest.
And then there is your body.
I have begun to realize that my endocrine responses are not standard. My ovaries do not react exactly as expected. My hormonal shifts hit hard. The feedback loops feel exaggerated. And now, during downregulation, the water retention and systemic changes are intense.
When you live with lipedema, you already know hormones matter.
Puberty. Pregnancy. Perimenopause. Hormonal contraception.
These are not neutral events.
Across multiple cohorts, women with lipedema frequently report cycle related symptoms and diagnoses that originate from the ovaries and the menstrual system.
That pattern deserves attention.
What the study actually found about ovaries and lipedema
The most concrete finding comes from the largest cohort included in the review, a Spanish study of 1803 women with lipedema.
In that cohort, 76 percent of women were described as having what the authors called inflammatory ovarian dysfunction.
That phrase sounds dramatic. But the review carefully clarifies that this is not a standardized gynecologic diagnosis. It was a clinically defined symptom cluster based on medical history and records. It included irregular cycles, heavy menstrual bleeding, and pelvic pain. My cycles are normal, I have no pain, and this does not align with my history. My history shows highly fluctuating AMH and AFC levels, which are typically expected to be relatively stable.
In other words, it reflects patterns of ovarian and menstrual disturbance, not a single disease.
The review also summarizes that PCOS appears in lipedema cohorts at rates around 12 to 17 percent in the datasets examined. Ovarian cysts are reported in some cohorts. Infertility is reported by a proportion of women, often as self reported history rather than a clearly defined cause.
What this means is not that lipedema causes PCOS.
Not that lipedema causes infertility.
Not that the ovaries are dysfunctional because of lipedema.
What it means is this.
In populations of women diagnosed with lipedema, often recruited from specialist care, there is a high frequency of cycle related complaints and some ovarian related diagnoses. The authors suggest this fits into a broader endocrine and inflammatory framework in which lipedema clusters with hormone sensitive traits across life stages, particularly puberty, pregnancy, and menopause.
At the same time, they are explicit.
The evidence is heterogeneous.
Many outcomes are symptom based.
There is no proof of causality.
This is a pattern. Not a verdict.
Artificial menopause and the body I do not recognize
Right now, I am living inside a hormonal experiment.
Decapeptyl contains triptorelin, a GnRH agonist. It first creates a short flare, a temporary surge of gonadotropins and estrogen. Then it shuts the system down. LH and FSH fall. Estrogen drops. The body enters a temporary, drug induced menopause.
This rapid hormonal shift affects multiple systems at once.
It is common to experience increased fluid retention after depot downregulation.
Mechanistically, several things are happening at the same time.
The initial flare phase can itself cause water retention.
The subsequent rapid estrogen drop alters vascular tone and capillary permeability. Some women become more edema prone when estrogen falls quickly.
Progesterone balance shifts as well. Progesterone normally has a mild diuretic effect through antagonism of aldosterone. When that balance is disrupted, fluid can be retained more easily.
In fertility treatment, this water retention is often most pronounced in the first two to three weeks after the depot injection and then stabilizes. For some women, it persists through the entire downregulation phase.
Understanding this intellectually does not make it easier emotionally.
When you live with lipedema, water is not neutral. Swelling is not neutral. Hormonal fluctuation is not abstract. It is visible. It is tangible. It changes how you move through the world.
Seeing my body hold this much fluid has been confronting in a way I did not anticipate. It feels like every endocrine lever in my system has been pulled at once.
The gut, estrogen, and feeling unwell
Low estrogen does not only affect fat and vessels. It also affects the gut.
Estrogen interacts with receptors in the nervous system and the intestinal wall. When estrogen falls rapidly, gut motility can slow. Peristalsis becomes less efficient. Constipation becomes more likely. Stool can become drier.
At the same time, fluid shifts and electrolyte changes can alter how water is distributed between tissues and the intestinal lumen.
Many women in downregulation describe a general sense of unwellness that includes fatigue, headaches, mild nausea, bloating, mood changes, and abdominal pressure.
It is, in practice, a sudden endocrine reset.
There is also growing research on the estrobolome, the subset of gut bacteria that participates in estrogen metabolism. Certain bacteria produce beta glucuronidase and other enzymes that influence how much estrogen is deconjugated and reabsorbed in the enterohepatic circulation.
In low estrogen states, shifts in microbiota composition and enzymatic activity are observed. The strongest evidence is mechanistic and associative. Clinical interventions targeting the microbiota specifically for low estrogen constipation or edema are still an evolving field.
Practically, what helps in this phase is often very simple.
Gradual increase in fluid intake.
Careful, not aggressive, fiber adjustment.
Psyllium when hydration is stable.
If motility is already slow, an osmotic agent such as macrogol can be more effective than simply adding more fiber.
Regular gentle movement.
Consistent meal timing.
Sleep as best as possible.
Stability matters because stress and the brain gut axis strongly influence motility.
Probiotics and fermented foods are individual. Some women feel better. Others feel more bloated. Mechanistically the microbiota estrogen connection is interesting, but we do not yet have robust clinical data showing one specific probiotic strategy consistently resolves low estrogen constipation.
So where does lipedema fit into all this
This is the question I keep returning to.
The review does not say that lipedema causes ovarian disease. It does not say that ovarian markers like AMH or AFC are systematically altered in lipedema. It does not say IVF outcomes are worse.
What it does suggest is that lipedema often coexists with hormone sensitive patterns across life.
Onset around puberty.
Worsening during pregnancy.
Progression around menopause.
High rates of menstrual disturbances and pelvic pain in cohorts.
Notable frequency of PCOS and cysts in some datasets.
That does not prove a shared cause.
But it does support the idea that lipedema may be part of a broader endocrine sensitivity.
As I sit here in artificial menopause, swollen and unfamiliar to myself, I cannot ignore the possibility that my reproductive system and my adipose tissue have always been in dialogue.
Not enemies.
Not separate.
But part of the same endocrine terrain.
What this study does and does not allow me to conclude
It allows me to say that the overlap between lipedema and gynecologic symptoms is real enough to warrant serious research.
It allows me to say that clinicians should not dismiss pelvic complaints in women with lipedema as incidental.
It does not allow me to say that my ovarian response in IVF is impaired because of lipedema.
It does not allow me to say that lipedema is an ovarian disease.
It allows me to say there is a pattern.
And patterns deserve structured investigation.
The authors are clear that we need prospective studies with standardized gynecologic evaluation. We need consistent diagnostic criteria. We need molecular profiling across phenotypes.
Until then, we are working with signals.
Living in the middle of the signal
Right now, this is not theoretical for me.
It is waking up feeling swollen.
It is wondering whether the next phase of stimulation will feel better or worse.
It is watching my body respond differently than expected.
It is holding grief and hope at the same time.
It is also recognizing that lipedema has never been only about fat.
It has always been about hormones, inflammation, vascular behavior, tissue remodeling, pain signaling, and life stage transitions.
This study does not give me an answer about my ovaries.
But it gives me something else.
It gives me language for the possibility that what I am experiencing is not random. That the endocrine sensitivity I see in my legs may also exist in my reproductive system. That my body’s reactions are coherent, even when they are inconvenient.
And maybe that is the beginning of a more integrated way of understanding women’s bodies.
Not compartmentalized.
Not dismissed.
But taken seriously, in full complexity.
Read the study here:
When Lipedema and Gynecologic Health Collide

If you live with lipedema, you probably do not need a scientist to tell you that your body reacts to hormonal seasons. Puberty. Pregnancy. Perimenopause. Sometimes birth control. Many women can point to a very specific window when their legs changed, pain started, bruising became constant, or swelling became harder to manage.