
What Do We Really Know About Lipedema in Men?
Why male lipedema matters, what the newest case series reveals, and why expanding the picture of this disease may help us understand lipedema better for everyone.

Over the past few years, I have spoken with hundreds of women with lipedema. Several have told me about male family members who seem to have the same symptoms that we, as women with lipedema, experience. Lipedema is often described as a women’s disease, typically emerging during hormonal phases such as puberty. But the more people I speak with, the more I realize how much we still do not know about lipedema. We have only just begun to see the outlines of what future research may reveal.
For example, lipedema is often described as a symmetrical disease that affects both sides of the body equally. That has never been true for my lipedema. I have always been more severely affected on the right side of my body. In fact, this was the only reason I was referred to the right specialist and diagnosed with lipedema as early as 2012.
For a long time, I had struggled with unexplained pain in my legs. My mother has ME and experiences aching in her body because of her illness. I remember very clearly a conversation we had on the stairs in my childhood home. I was so distressed by the pain in my legs, and it was so bad that it affected my sleep. Before going to bed, I had to massage my thighs and calves to ease the pain. My mother also told me about the aching she experienced in her own body, and I began to worry that I might have ME too. These were the fears of a young girl living with pain and trying to understand what her symptoms meant.
I do not have ME. My aching came from something different than my mother’s.
I was in and out of the doctor’s office, and my wonderful GP was clearly frustrated that she could not help me or give me answers. But she tried. She prescribed diuretics because she could see that my calves were swollen, but they did not help. She noticed that my right calf was slightly larger than my left and brought out a measuring tape. She wanted to rule out a blood clot and referred me for assessment at the vascular department of a Norwegian hospital.
The doctor I met there immediately recognized that it was lipedema.
I have always had a very disproportionate body, with a very small upper body and much wider hips. The shape of my body itself was never something I felt insecure about. In my teens and twenties, I was actually proud of my curves. The problem was the pain. It was obvious that something inside the tissue of my body was not quite right.
At the hospital, the doctor showed me what my fat tissue looked like on ultrasound in different areas of my body. I left the appointment with only a few short messages. There was nothing to do about it. I should maintain my current weight. I should use compression. I had just turned 20, and at that time, no one had heard of lipedema. Compression stockings did not feel like a realistic option back then. He also told me never to consider surgery because it could make things worse.
Regarding his comment about surgery, I do not know exactly what he meant. This was 14 years ago, so my interpretation today is that the methods used in 2012 may not have been good enough for lipedema patients, and that there may have been a risk of developing secondary lymphedema. But that is only my assumption.
So yes, my lipedema has never been symmetrical. When I had lipedema surgeries in 2021 and 2022, the surgeon removed more fat from my right side.
This brings me to the topic of this article.
For a long time, lipedema has been described as a disease that almost exclusively affects women. This is understandable, because the vast majority of people diagnosed with lipedema are women, and because the disease often begins or worsens during hormonal life stages such as puberty, pregnancy and menopause.
But this does not mean that men cannot have lipedema. It may simply mean that men with lipedema have been even more invisible.
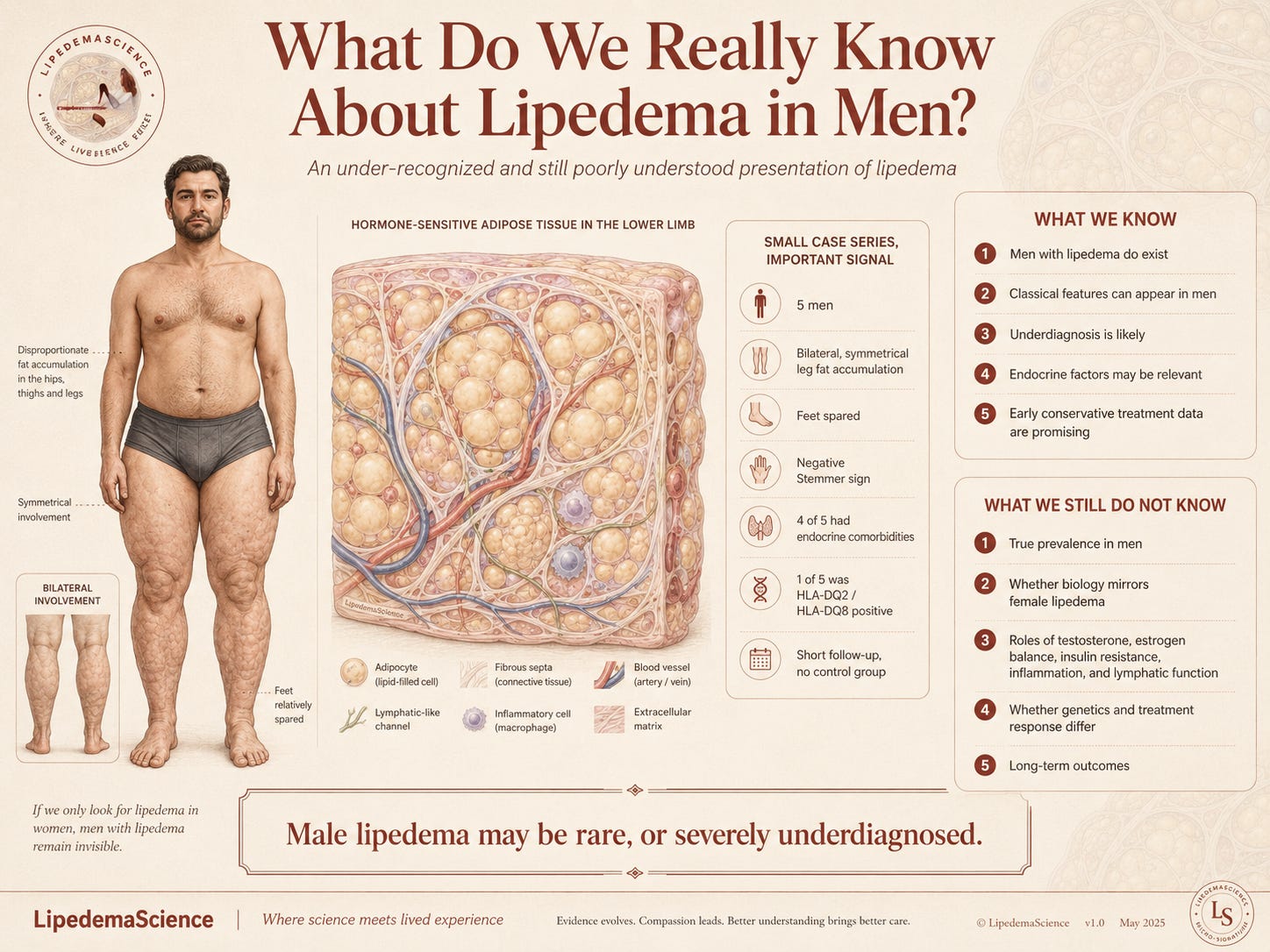
A new case series from the Amato Institute of Advanced Medicine in São Paulo describes five men with lipedema. All of them had classical clinical features, including bilateral and symmetrical fat accumulation in the legs, disproportionate fat distribution, sparing of the feet and a negative Stemmer’s sign. This matters because it shows that men can present with a clinical picture similar to what we recognize in women with lipedema.

The study does not show that we now understand lipedema in men. But it does show that men with lipedema exist, and that they deserve to be taken seriously.
What we know is that lipedema in men appears to be rare, or at least severely underdiagnosed. We also know that men can have classical lipedema features, and that some reported cases are associated with endocrine or metabolic conditions. In this case series, four out of five men had endocrine comorbidities. This fits with the hypothesis that hormonal regulation may be particularly relevant when lipedema occurs in men.
At the same time, we need to be careful. We do not yet know whether these hormonal findings are a cause, a trigger, a risk factor or simply conditions that happen to occur at the same time.
We also do not know how common lipedema in men really is. When a disease is defined as almost exclusively female, healthcare professionals are less likely to look for it in men. Men with painful, disproportionate fat distribution in the legs may therefore be more easily dismissed as having overweight, obesity, lymphedema or simply an unusual body type. This may mean that many never receive a proper assessment.
What we do not know is whether lipedema in men has the same biological mechanisms as lipedema in women. We do not know whether the disease develops in the same way, whether the pain profile is the same, whether genetic factors play the same role, or whether treatment should be adapted differently. We also do not know enough about the role of testosterone, estrogen balance, insulin resistance, inflammation, lymphatic function or the immune system in men with lipedema.
In this study, one of the men tested positive for HLA DQ2 and HLA DQ8, which the authors present as a possible immunological clue. This is interesting, but it must be interpreted cautiously. One positive patient in a series of five is not enough to conclude that lipedema in men is autoimmune or gluten related. It is a research clue, not a conclusion.
The same applies to the treatment results. The patients lost weight and had reduced leg volume after four to eight weeks of conservative treatment. This is promising, but we do not know how much of the volume reduction was due to loss of ordinary fat mass, fluid, edema, inflammation or changes in the lipedema tissue itself. The study had no control group and only short follow up, so the results should be understood as preliminary.
Still, this study matters. Not because it gives us all the answers, but because it opens a door. It reminds us that lipedema research is still young, and that we must be careful not to make the disease narrower than it really is. If we only look for lipedema in women, we will only find lipedema in women. If we never ask whether men can have lipedema, men with lipedema will remain invisible.
This is also about community. Women with lipedema already know what it feels like not to be believed, not to be understood and not to be studied enough. Men with lipedema belong to an even smaller and more invisible minority. They may face the same medical dismissal, but in addition, they may carry the shame of having a disease that is almost always described as female.
That is why we need to shine a light on lipedema in men. Not to shift attention away from women, but to expand our understanding of the disease. When we include men, we may also learn more about the biology of lipedema in general. Male cases may provide important insights into hormonal mechanisms, genetic vulnerability, fat tissue regulation and inflammation. They may help us understand why lipedema develops, why it affects people differently and which mechanisms truly drive the disease.
Embracing men with lipedema is therefore both humanly and scientifically important. No one with lipedema should be left outside simply because their body does not fit the picture that research has focused on so far.
Do you know a man with lipedema? Share this article with him.