
Tirzepatide, Inflammation, and Fibrosis
A science dive sparked by your questions.

One of the things I value most about running this platform is the quality of the questions you ask.
 single-dose vials ...")
Many of them arrive in my inbox long before there are clear answers in the scientific literature. Sometimes there is no data at all, only lived experience, shared patterns, and recurring observations from people with lipedema. That is often how science actually begins. First as patient experience. Then as a hypothesis. And sometimes, if the signal is strong enough, as a pilot study or a small clinical investigation.
For me, this is the real value of this space. It keeps me on a continuous growth path. Learning new things. Diving into unfamiliar mechanisms. Challenging my own assumptions. And, importantly, refining how I understand my own lipedema journey.
One question that keeps returning is this….
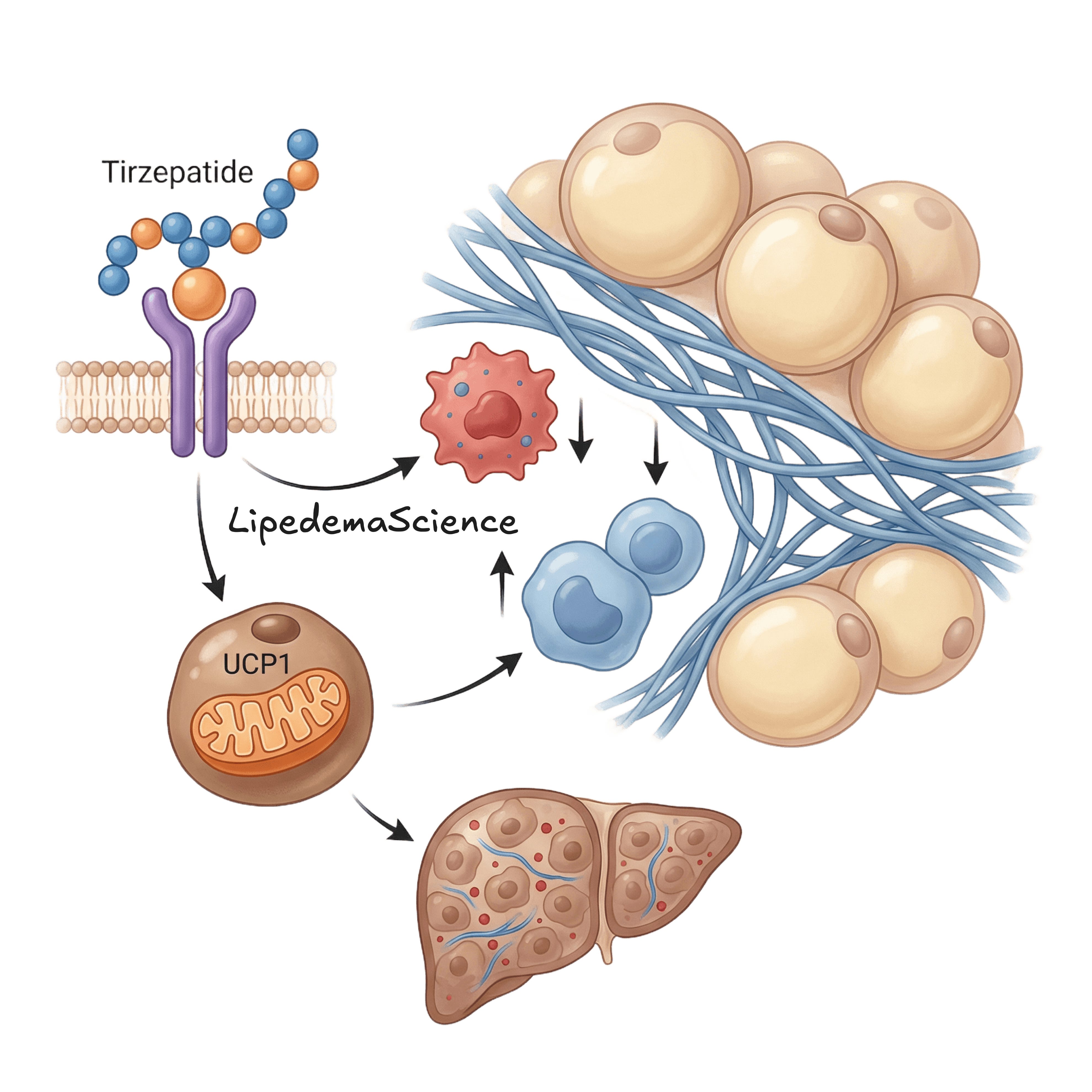
What do you think about tirzepatide as an aid for inflammation and fibrosis?
This time, the situation is different from many other topics we discuss here. There are studies. Not large randomized trials in lipedema yet, but enough mechanistic, translational, and early clinical data to make the question worth a serious scientific dive.
So let us do exactly that.
Why inflammation and fibrosis matter in lipedema
Lipedema is not just about excess fat. The condition is increasingly understood as a complex disorder involving adipocyte dysfunction, chronic low-grade inflammation, microvascular changes, pain signaling, and progressive extracellular matrix remodeling.
