
Lipedema Through Every Hormonal Season
What science knows – and still needs to learn – about puberty, pregnancy, breastfeeding, and menopause in women with Lipedema.

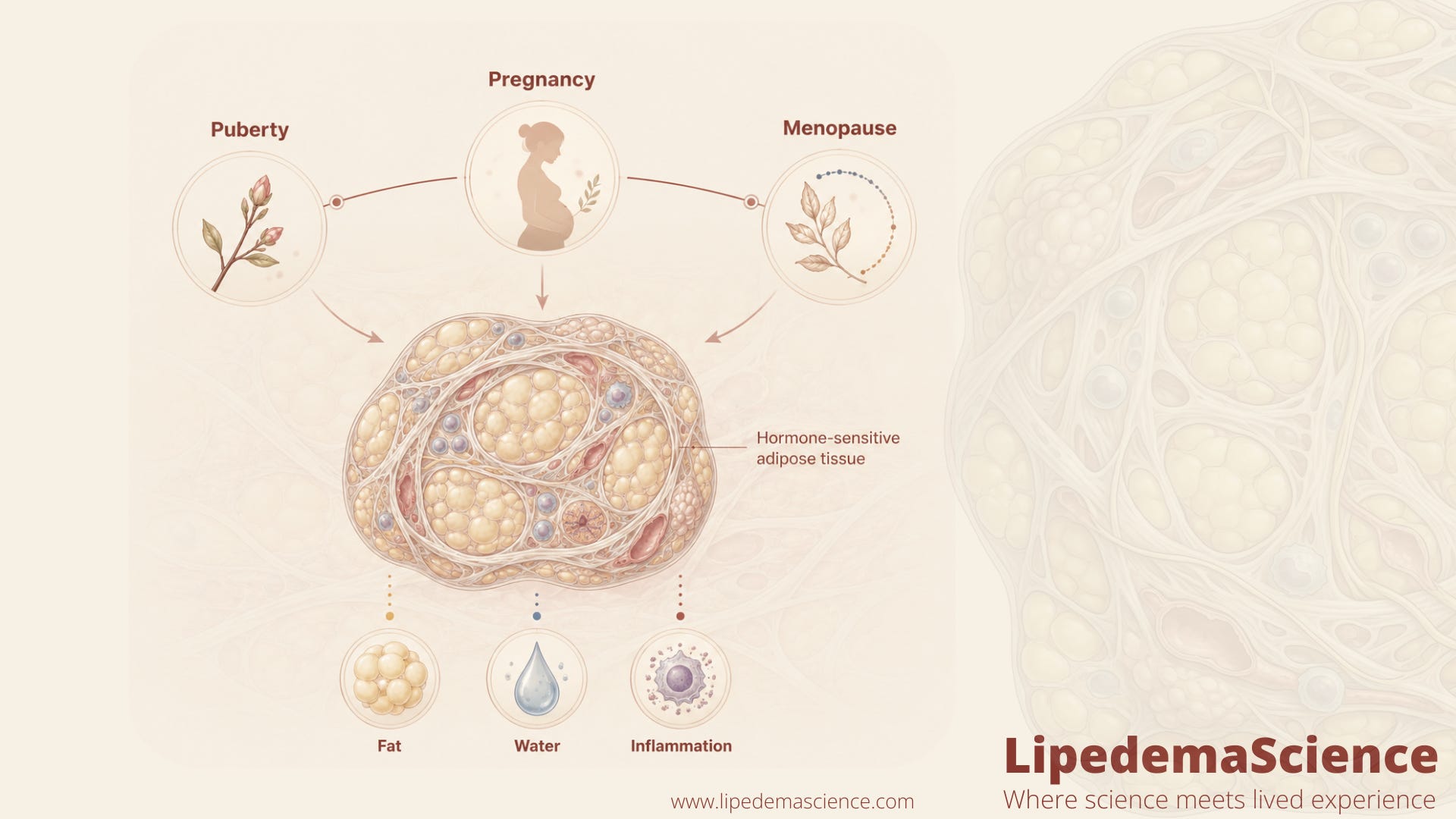
Hormones as Turning Points
For many women, lipedema doesn’t just appear — it arrives at key hormonal moments: puberty, pregnancy, or menopause. These transitions shape how the body handles fat, water, and inflammation. Scientists now believe these hormonal “seasons” aren’t random triggers, but windows when the body’s fat tissue becomes more responsive — or vulnerable — to estrogen signaling.
Across multiple studies, researchers describe lipedema as a hormone-sensitive fat disorder. A 2026 systematic review by Bertsch and colleagues, which looked specifically at the association between hormones and lipedema pathophysiology, concluded that lipedema appears to be a multifactorial condition primarily driven by hormonal dysregulation, especially involving estrogen, alongside metabolic and possible genetic components. The authors actually went further and argued that this evidence supports reclassifying lipedema as a hormonally influenced disorder distinct from obesity. That is a meaningful conceptual shift. It is not caused by hormones alone, but hormones seem to decide where and how the disease manifests. Yet, despite this clear pattern, the precise mechanisms — the molecular switches that turn sensitivity into swelling, or pain into chronicity — remain largely unknown.

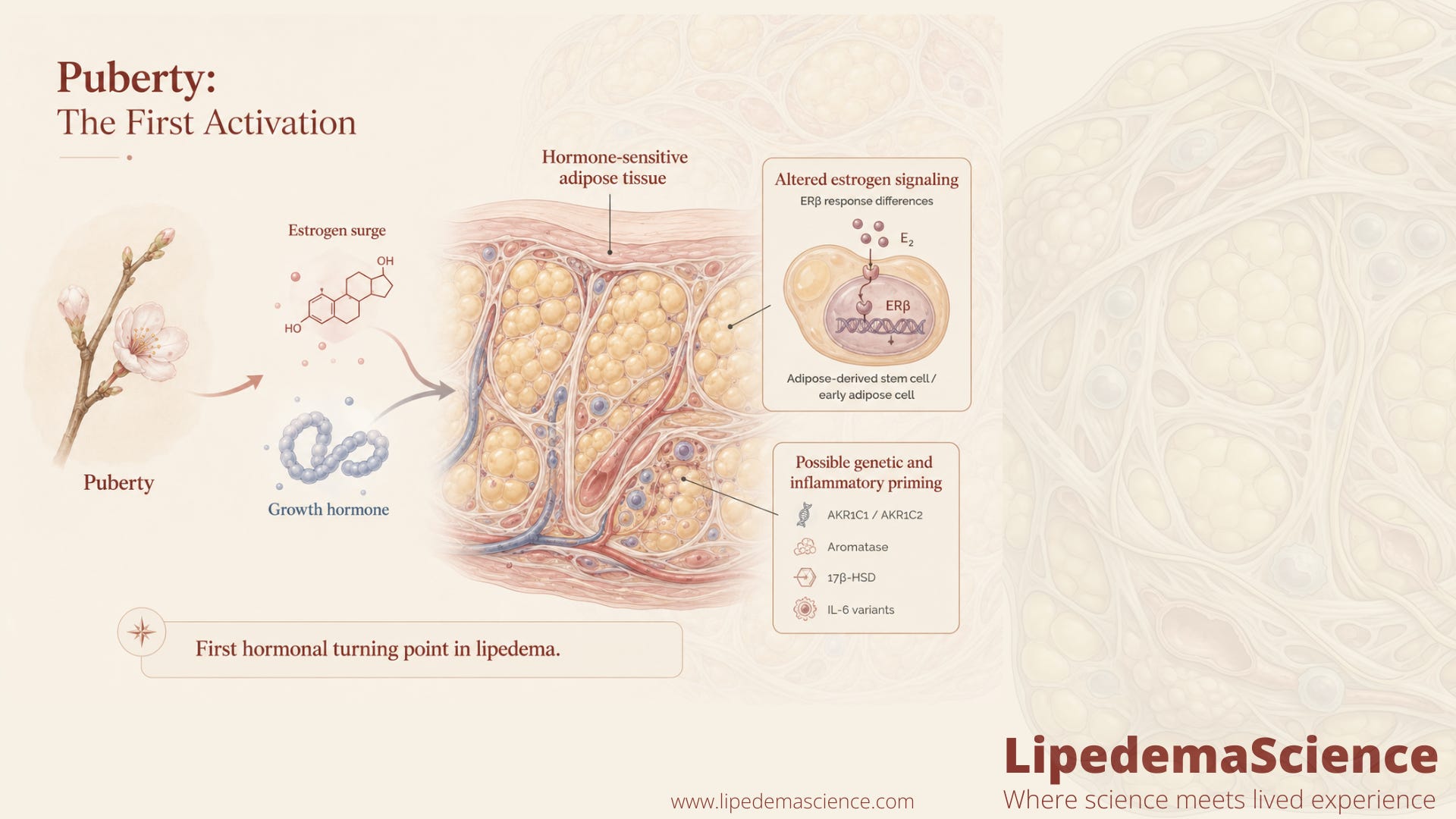
Puberty: The First Activation
Puberty is where lipedema often begins. The shift from childhood to reproductive maturity brings an explosion of estrogen and growth hormone, which reshape fat distribution throughout the body. In most girls, these changes give the characteristic feminine pattern — more fat in the hips and thighs, less around the abdomen.
But in some, this process overshoots. Research in human adipose-derived stem cells (ASCs) from women with lipedema, compared with healthy BMI- and age-matched controls, has shown that lipedema cells respond differently to estrogen exposure in the lab. In one study, ERβ expression was significantly higher in hormone-depleted lipedema ASCs and spheroids compared with healthy cells, while estrogen treatment downregulated ERα and GPER in lipedema spheroids. These are early in vitro findings and cannot be directly translated to what happens in a young girl’s thigh during puberty, but they support the broader hypothesis that lipedema fat is biologically wired to “read” estrogen signals differently from the start.
There’s still no definitive biomarker explaining why some girls develop lipedema and others do not. Genetic factors likely play a role. The literature has begun pointing toward steroid-metabolizing enzyme pathways, including AKR1C1 and AKR1C2, which are involved in progesterone and androgen handling, and toward aromatase activity, 17β-HSD enzymes, and connective tissue composition. One observational study has also reported that certain IL-6 gene polymorphisms (rs1800796 and rs1800795) appear more often in women with lipedema than in controls, especially in younger women, hinting that inflammatory signaling and hormone biology may both be genetically primed. None of these findings explains lipedema on its own, and replication is still limited. For now, puberty remains the first and most mysterious hormonal turning point.
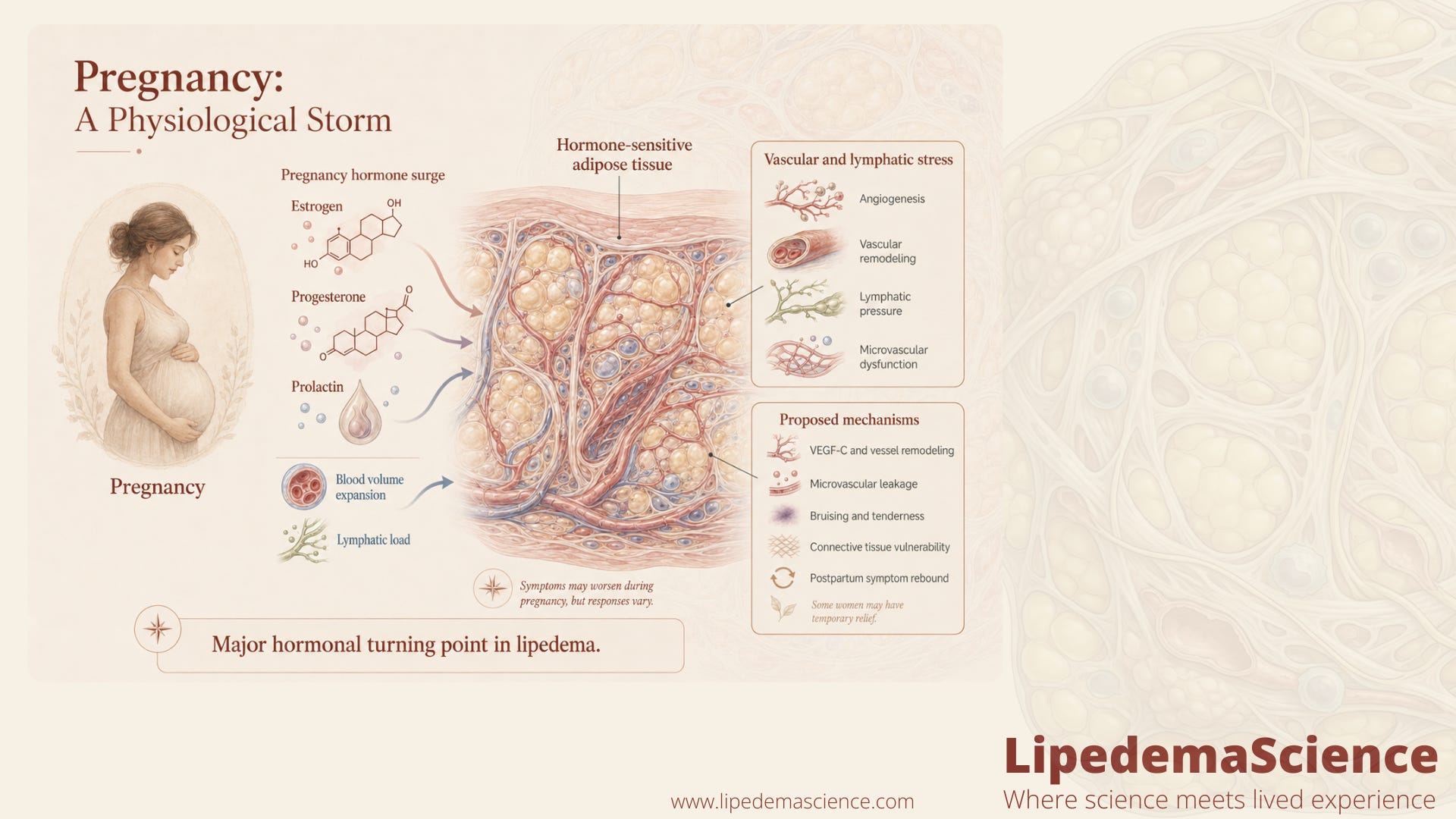
Pregnancy: A Physiological Storm
During pregnancy, estrogen, progesterone, and prolactin levels rise to extraordinary heights. Blood volume expands, tissues become more elastic, and the lymphatic system is under heavy pressure. For women with lipedema, this hormonal and circulatory stress can act as an accelerator: pain intensifies, swelling increases, and the legs feel heavier.
Pregnancy is consistently described in review papers as one of the three major hormonal windows — alongside puberty and menopause — when lipedema onset or worsening is observed. The mechanisms remain hypothesis-driven rather than directly proven in pregnant women, because almost no studies have followed lipedema biology longitudinally through gestation. What we do know from broader lipedema research is that the tissue shows signs of microvascular dysfunction and increased systemic VEGF-C, both of which are biologically relevant to pregnancy, when angiogenesis and vascular remodeling are at their peak.
Some studies suggest that the surge of estrogen-driven angiogenesis — the formation of new capillaries — combined with progesterone resistance in connective tissue may worsen microvascular leakage. This contributes to the bruising and tenderness typical of lipedema. It is important to be honest, though, that these are proposed mechanisms rather than confirmed pregnancy-specific findings.
Yet, not all women experience worsening during pregnancy; some even notice temporary relief. Why? One hypothesis is that high progesterone temporarily dampens inflammation and nerve sensitivity. But this balance is fragile — after birth, when hormones plummet, symptoms often rebound.
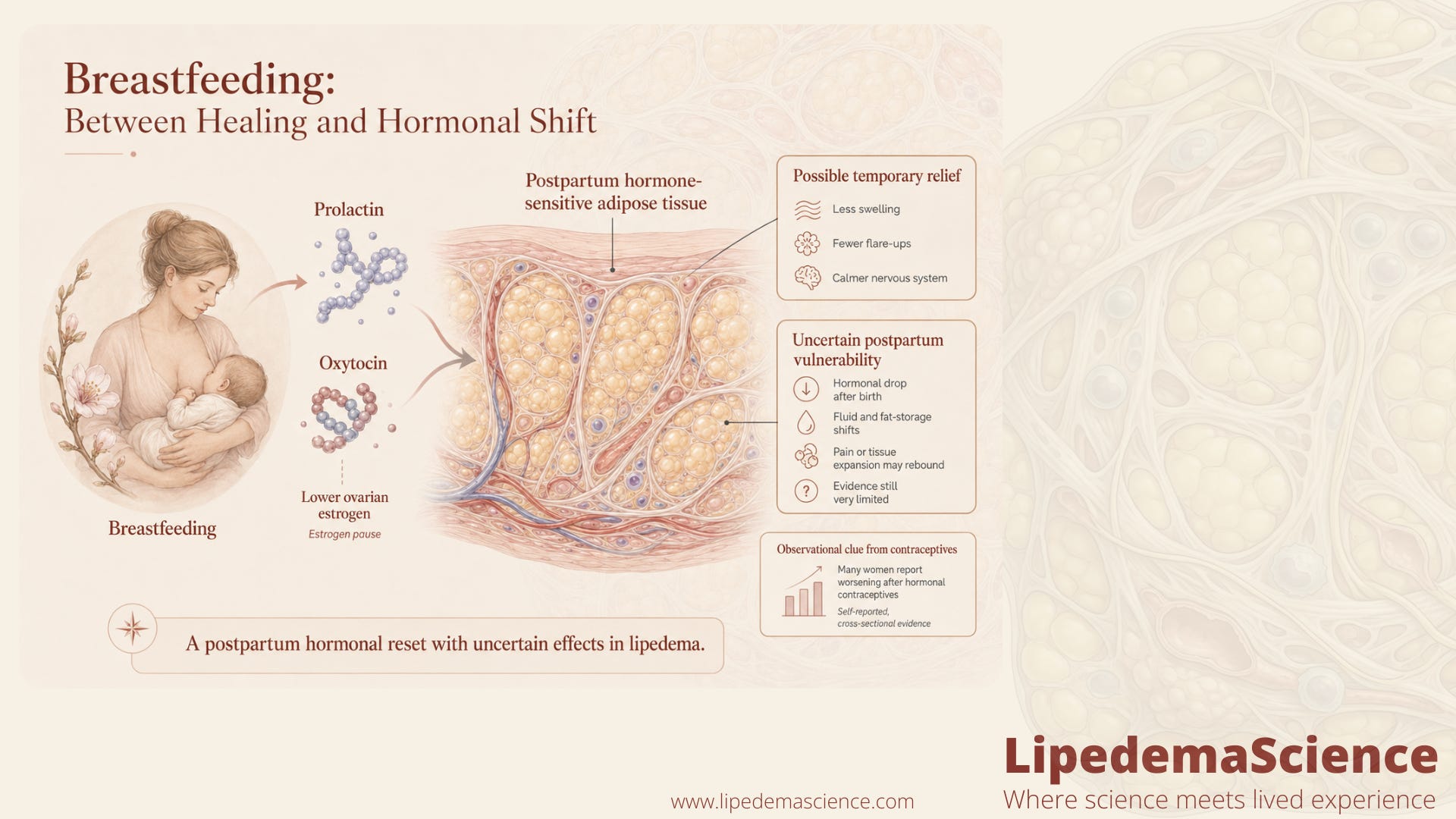
Breastfeeding: Between Healing and Hormonal Shift
After delivery, prolactin and oxytocin dominate. These hormones encourage milk production and calm the nervous system — but they also suppress ovarian estrogen. For some women, this estrogen “pause” feels like a break: less swelling, fewer flare-ups. For others, the sudden hormonal drop leaves the tissue vulnerable again, triggering renewed pain or expansion.
Research on breastfeeding and lipedema is still extremely limited. There are no dedicated PubMed-indexed studies on lipedema during lactation that I am aware of — only mentions within broader hormonal-context reviews. Scientists have yet to clarify whether breastfeeding offers protection, neutrality, or risk. What’s clear is that the postpartum period is another metabolic reset, when inflammation, fluid balance, and fat storage fluctuate dramatically. This is one of the clearest unanswered questions in the field and a real example of how much patient-relevant biology has simply not been studied yet.
A related and slightly better-studied area concerns exogenous hormones outside pregnancy. A 2025 cross-sectional study of 637 Brazilian women with suspected or confirmed lipedema reported that among those who had used hormonal contraceptives, 58.8% described symptom worsening after starting them (34.5% severe, 24.3% slight), while only 0.9% reported improvement. Around 15% reported that their lipedema symptoms started temporally around contraceptive initiation. This is observational, self-reported, and cross-sectional, so it cannot prove causation. But it does suggest that exogenous estrogen-progestin combinations interact with lipedema tissue in ways worth taking seriously — and worth discussing individually with a clinician.
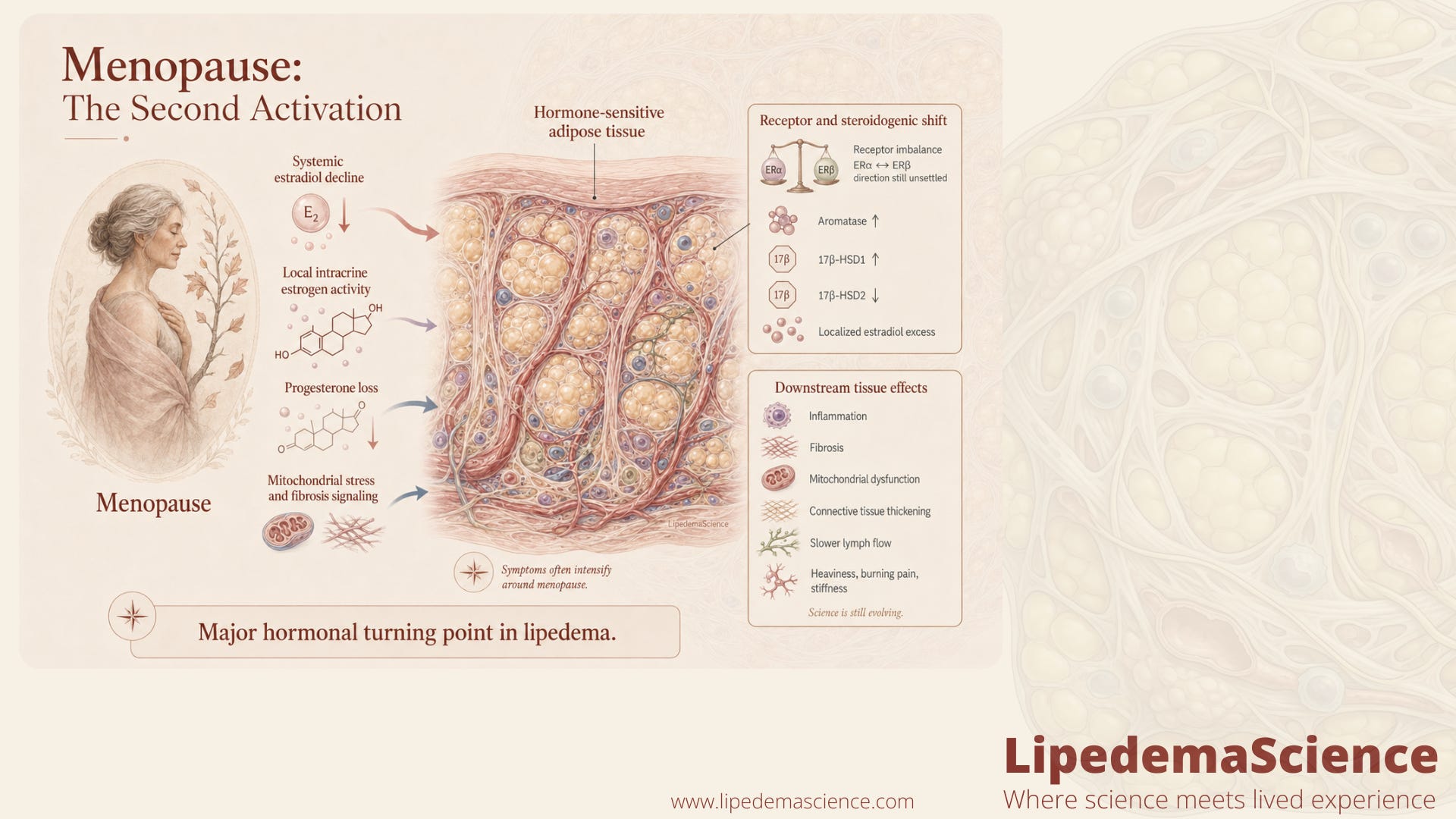
Menopause: The Second Activation
Menopause is the phase most consistently linked with worsening lipedema. As ovarian estrogen production declines, systemic estradiol drops — but paradoxically, lipedema tissue becomes more active hormonally. A 2025 narrative review proposed a detailed model in which menopause acts as a critical turning point in lipedema progression, driven by what the authors describe as estrogen receptor imbalance, intracrine estrogen excess, and adipose tissue dysfunction. According to this model, the upregulation of aromatase and 17β-HSD1, combined with suppression of 17β-HSD2, sustains a localized estradiol excess inside the fat tissue itself, even when blood estrogen is low.
Here it is worth flagging an honest contradiction in the literature. One major review describes the menopausal shift as ERβ predominance over ERα, with this pattern linked to inflammation, fibrosis, and reduced mitochondrial function. Another review on the hormonal links between lipedema and gynecological disorders describes the imbalance the other way around, as ERα dominance over ERβ. Both papers connect estrogen receptor imbalance to inflammation, hypertrophy, microangiopathy, immune dysfunction, and fibrosis — but the direction of the imbalance is not yet settled. This is exactly the kind of detail where the science is genuinely evolving, and we should not pretend otherwise.
What does seem more consistent across studies is that the receptor landscape itself shifts at menopause, that local steroidogenic enzyme activity increases in lipedema adipose tissue, and that these changes are tied to inflammation, fibrosis, and impaired mitochondrial function. This may help explain why symptoms such as heaviness, burning pain, and tissue stiffness often intensify around menopause.
Another layer is the loss of progesterone’s protective tone. When estrogen becomes unopposed, connective tissue thickens, lymph flow slows, and inflammation deepens. It’s not just the loss of hormones that matters — it’s which receptors remain active and where.
Why These Patterns Matter
Across all hormonal stages, one truth keeps returning: lipedema fat behaves as if it has its own endocrine life. It produces, stores, and responds to hormones differently than normal tissue. Even when blood levels of estrogen are low, the fat itself can generate estradiol locally through aromatase and 17β-HSD1 activity. This may explain why standard hormone tests often look normal — the imbalance happens inside the tissue, not in the bloodstream.
A recent scoping review that synthesized 25 studies across ten countries reinforced this picture, concluding that lipedema clusters with hormone-sensitive gynecologic and endocrine features across reproductive life stages, and that the field is shifting from a primarily lymphovascular paradigm toward a more integrated endocrinometabolic framework. That shift matters clinically, because it changes what we are trying to measure, treat, and validate.
Understanding these localized hormonal processes — known as intracrinology — could open new treatment pathways. Instead of adjusting systemic hormones, future therapies might target the enzymes and receptors within the fat itself, restoring the body’s ability to respond to signals in balance.
What Science Still Doesn't Know
Despite major advances, there’s much we still don’t know. Researchers are only beginning to map the receptor distribution (ERα, ERβ, GPER) in lipedema tissue across different life stages. We also lack longitudinal studies that follow women from puberty to menopause to track how symptoms evolve with hormonal milestones. Most of the existing hormone-and-lipedema literature is observational, cross-sectional, or based on small tissue samples and in vitro experiments. Many studies are not yet replicated. Sample sizes are often modest, and BMI- and age-matched controls are not always included.
We don’t yet understand:
Why lipedema almost exclusively affects women.
Whether early hormone modulation could prevent progression.
How genetic polymorphisms in estrogen-related genes, IL-6, and steroid-metabolizing enzymes such as AKR1C1 shape individual risk.
Whether menopausal hormone therapy can stabilize, rather than worsen, symptoms — and which types, doses, and routes are safest.
Whether breastfeeding meaningfully influences lipedema progression, symptoms, or remission.
Whether the receptor imbalance is truly ERβ dominant, ERα dominant, or context-dependent across stage, BMI, age, and tissue depot.
The next decade of research will need to combine molecular biology, imaging, and patient-reported data to connect the dots between hormone shifts, fat biology, and lived experience.
Looking Ahead: Toward Hormonal Precision Medicine
Lipedema challenges the idea that fat is passive. Instead, it is hormonally intelligent — and, in lipedema, overly responsive. The key for the future will be learning how to rebalance this sensitivity rather than suppress it.
That could mean developing therapies that fine-tune estrogen receptor signaling, strengthen progesterone pathways, or regulate local aromatase activity. Some early hypothesis-generating work has even raised the possibility that compounds such as resveratrol, or steroidogenic-targeted drugs like gestrinone and drospirenone, may eventually become relevant — but the direct lipedema evidence for any of these is still very limited and largely theoretical. It may also mean identifying biomarkers that predict which women are at risk of lipedema flares during hormonal transitions — from puberty to pregnancy to menopause.
In other words, science’s task is not only to understand hormones as triggers but to see them as guides — revealing how the body tries to adapt, and how, with the right support, it might one day find balance again.
Management of Lipedema with Ketogenic Diet: 22-Month Follow-Up (DOI: 10.3390/life11121402)
Observational Study on a Large Italian Population with Lipedema: Biochemical and Hormonal Profile, Anatomical and Clinical Evaluation, Self-Reported History (DOI: 10.3390/ijms25031599)
Lipedema and the Potential Role of Estrogen in Excessive Adipose Tissue Accumulation (DOI: 10.3390/ijms222111720)
Lipedema: From Women’s Hormonal Changes to Nutritional Intervention (DOI: 10.3390/endocrines6020024)
Reproductive Landmarks and Lipedema: Lessons to be Learned about Women Hormones throughout Life (DOI: 10.5772/intechopen.1006956)
Estrogen as a Contributing Factor to the Development of Lipedema (DOI: 10.5772/intechopen.96402)
Menopause as a Critical Turning Point in Lipedema: The Estrogen Receptor Imbalance, Intracrine Estrogen, and Adipose Tissue Dysfunction Model (DOI: 10.3390/ijms26157074)
Lipedema as a Hormone-Driven Gynecological Disorder: The Estrogen Receptor Connection (DOI: 10.5772/intechopen.1012036)
The Expression of Adipogenic Marker Is Significantly Increased in Estrogen-Treated Lipedema Adipocytes Differentiated from Adipose Stem Cells In Vitro (DOI: 10.3390/biomedicines12051042)
Impact of Hormones on Lipedema Development: A Systematic Literature Review (DOI: 10.1007/s00404-026-08318-1)
Reproductive Landmarks and Lipedema: A Scoping Review (DOI: 10.1177/02683555251410009)
Association Between Hormonal Contraceptive Use and Lipedema: A Cross-Sectional Study With 637 Brazilian Women (DOI: 10.7759/cureus.78234)
Aldo-Keto Reductase 1C1 (AKR1C1) as the First Mutated Gene in a Family with Nonsyndromic Primary Lipedema (DOI: 10.3390/ijms21176264)
Aldo-Keto Reductase 1C2 (AKR1C2) as the Second Gene Associated to Non-Syndromic Primary Lipedema (DOI: 10.26355/eurrev_202403_35776)
Capillary Western Immunoassay Optimization of Estrogen Related Factors in Human Subcutaneous Adipose Tissue (DOI: 10.1089/lrb.2022.0014)
Hormonal Links between Lipedema and Gynecological Disorders: Therapeutic Roles of Gestrinone and Drospirenone (DOI: 10.3390/ijms26094553)
Lipedema and Adipose Tissue: Current Understanding, Controversies, and Future Directions (DOI: 10.1097/SAP.0000000000004124)
Is Subcutaneous Adipose Tissue Expansion in People Living with Lipedema Healthier and Reflected by Circulating Parameters? (DOI: 10.3389/fendo.2024.1370646)
The Role of IL-6 Gene Polymorphisms in the Risk of Lipedema (DOI: 10.26355/eurrev_202004_20905)
Veldig spennande! Men samtidig veldig skummelt å stå med beina planta i dette i overgangsalderen!