
The Truth About Fat, Hormones and the Female Body
Why so many women with lipedema feel confused about metabolism, low-fat dieting, energy and hormonal health.

The Confusing Relationship Between Fat and Female Health
For many women with lipedema, the relationship with body fat becomes psychologically and biologically complicated long before they understand the condition itself. Puberty changes the body rapidly. Fat accumulates disproportionately around the legs, hips or arms. Pain, heaviness and swelling appear gradually. Some women notice dramatic worsening during pregnancy, hormonal contraception, fertility treatment or menopause. Others spend years trapped in cycles of restrictive dieting, overtraining and guilt around food, often without understanding why their body seems to respond differently than expected.
At the same time, modern nutrition culture sends deeply conflicting messages to women. For decades, dietary fat was framed as something dangerous that should be minimized. Grocery stores filled with low-fat yogurts, low-fat desserts, “light” products and heavily processed diet foods marketed as healthy choices for women. Simultaneously, another narrative emerged online saying that women “need fat for hormones,” often presented in an oversimplified and equally misleading way.
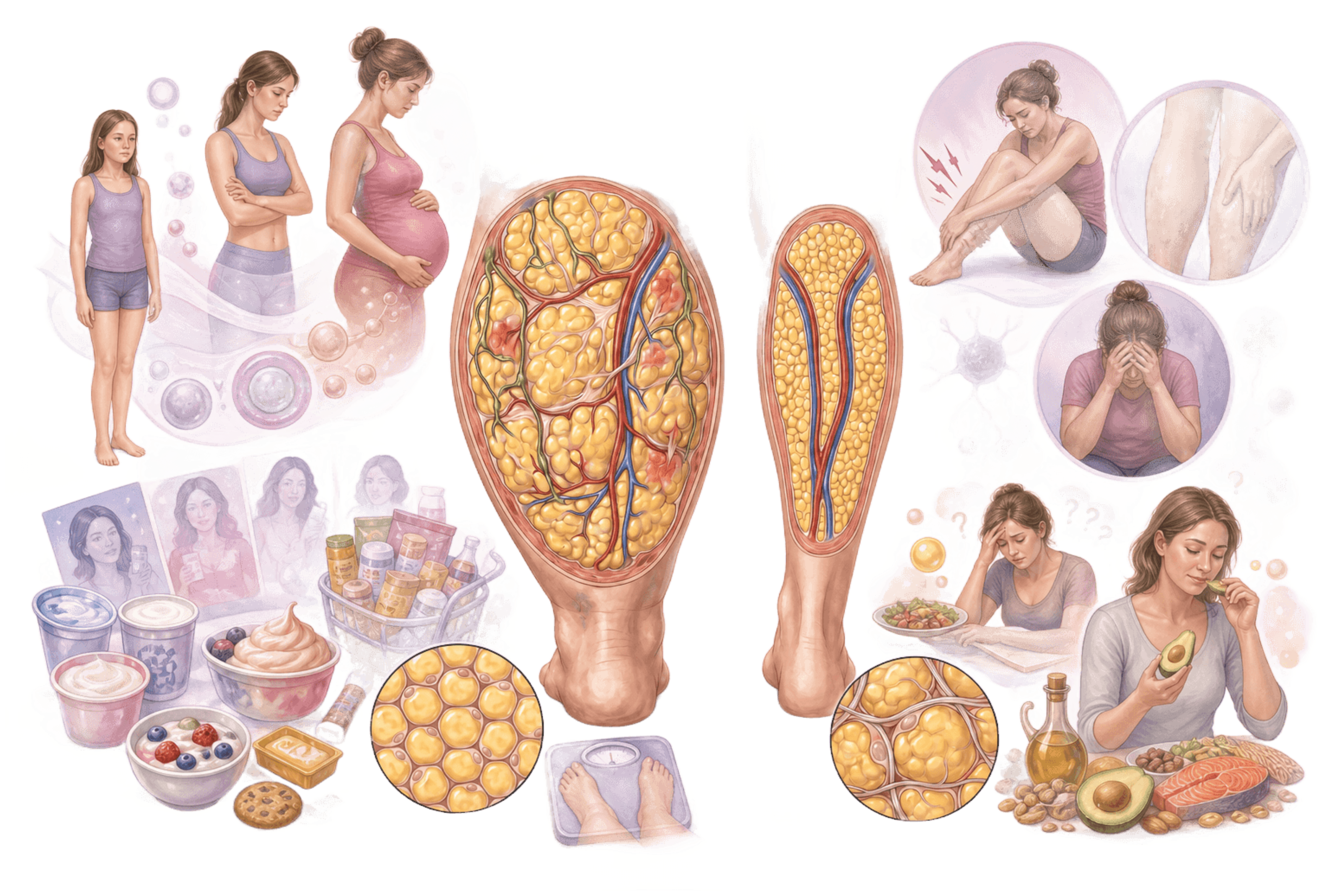
Women with lipedema frequently find themselves caught between these extremes. Many have spent years trying to lose fat aggressively while simultaneously noticing that hormonal changes seem to influence their symptoms profoundly. Some develop fear around eating fat altogether. Others begin to believe that eating more fat will somehow “fix hormones.” Neither explanation captures the complexity of female endocrinology.
What modern research actually shows is far more nuanced and far more interesting.


Female Hormones Are Not Controlled by One Single Factor
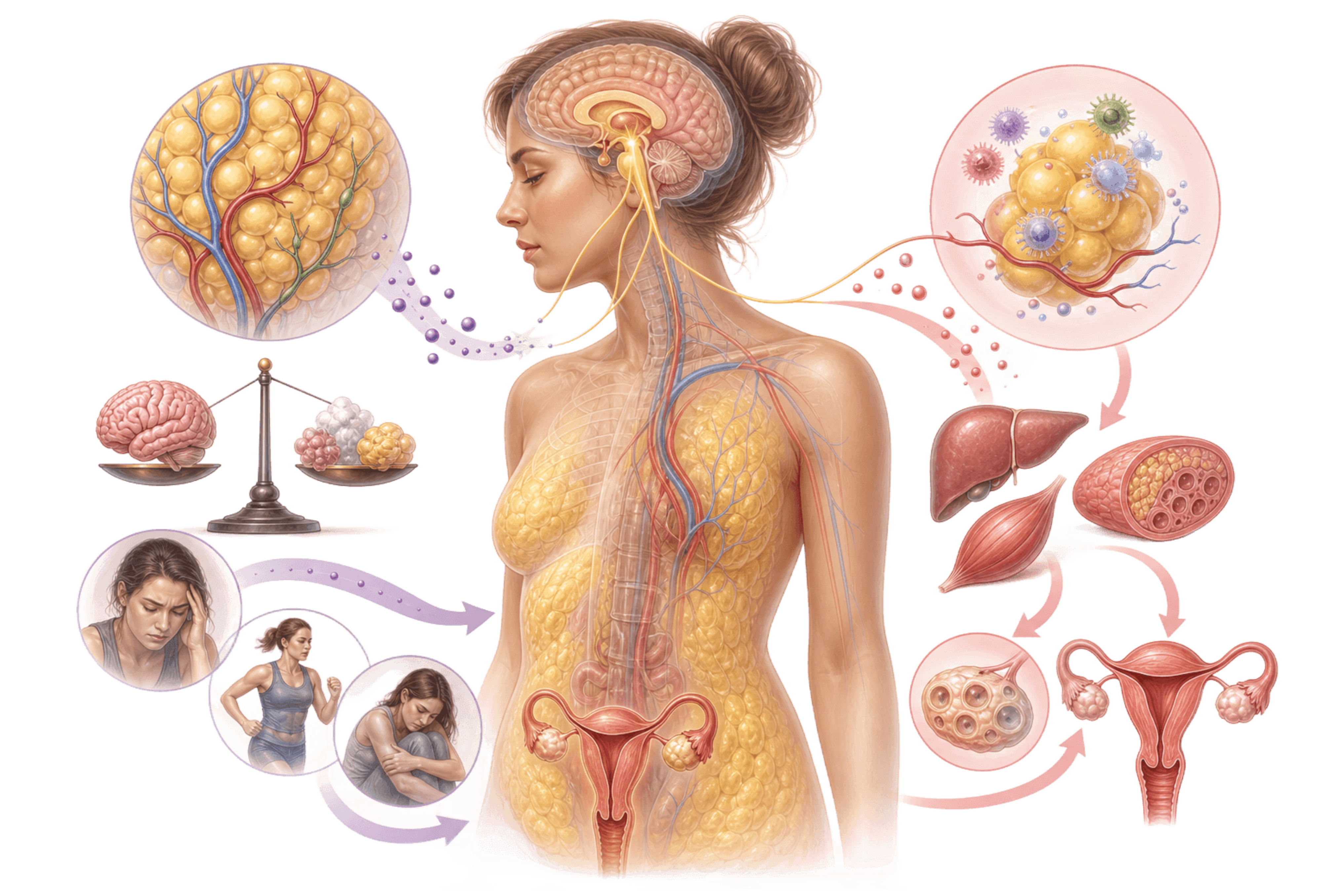
The female reproductive system is not controlled by a single nutrient, a single hormone or a single body composition measurement. Instead, it operates through a highly integrated network involving the brain, ovaries, adipose tissue, stress systems, metabolic signaling pathways and energy availability. Body fat itself is not merely passive storage. Adipose tissue functions as an active endocrine organ that continuously communicates with the hypothalamus, pituitary gland, immune system and reproductive axis. This becomes especially relevant in lipedema because lipedema exists within a hormonally sensitive, inflammatory and metabolically dynamic environment.
One of the most repeated statements in women’s health is that female hormones are “made from fat.” Biochemically, this is only partially true. The primary ovarian sex hormones such as estradiol and progesterone are steroid hormones synthesized from cholesterol. Steroid-producing cells obtain cholesterol through multiple pathways, including uptake from circulating lipoproteins, intracellular cholesterol stores and de novo synthesis. In other words, the body is not literally melting body fat into estrogen in a simplistic mechanical way.
The more clinically relevant point is that reproductive function is highly sensitive to energy status and adipose-derived signaling. Research over the past several decades suggests that many cases of hormonal dysfunction associated with restrictive eating, excessive exercise or significant weight loss are driven less by “running out of hormonal raw materials” and more by neuroendocrine adaptation. The brain continuously evaluates whether the body perceives the environment as metabolically safe enough to support reproduction.
This distinction matters enormously.
Energy Availability Matters More Than Most Women Realize
A woman can have relatively low body fat and still maintain normal reproductive function if energy availability, stress regulation and neuroendocrine signaling remain stable. Conversely, another woman may develop menstrual dysfunction despite not appearing extremely lean. In modern endocrinology, this is one reason why researchers increasingly focus on energy availability rather than body weight alone.
Some of the strongest experimental evidence comes from work by Anne Loucks and colleagues, who demonstrated that relatively short-term reductions in energy availability could disrupt luteinizing hormone pulsatility in healthy menstruating women. This research later became foundational for concepts such as Relative Energy Deficiency in Sport, often abbreviated RED-S. However, one of the most misunderstood aspects of this literature is the tendency to treat numerical thresholds as universal biological laws. The frequently cited value of approximately 30 kcal per kilogram fat-free mass per day originated from relatively small experimental studies and should not be interpreted as a rigid cutoff that applies identically to every woman. Later research and recent consensus statements emphasize considerable individual variation, methodological limitations in measuring energy availability and the importance of context.
This is particularly important in lipedema communities, where many women have histories of repeated restrictive dieting, chronic caloric deficits, appetite suppression, aggressive exercise or significant psychological stress around body image and food. The body does not respond solely to fat mass itself. It also responds to perceived energy sufficiency.


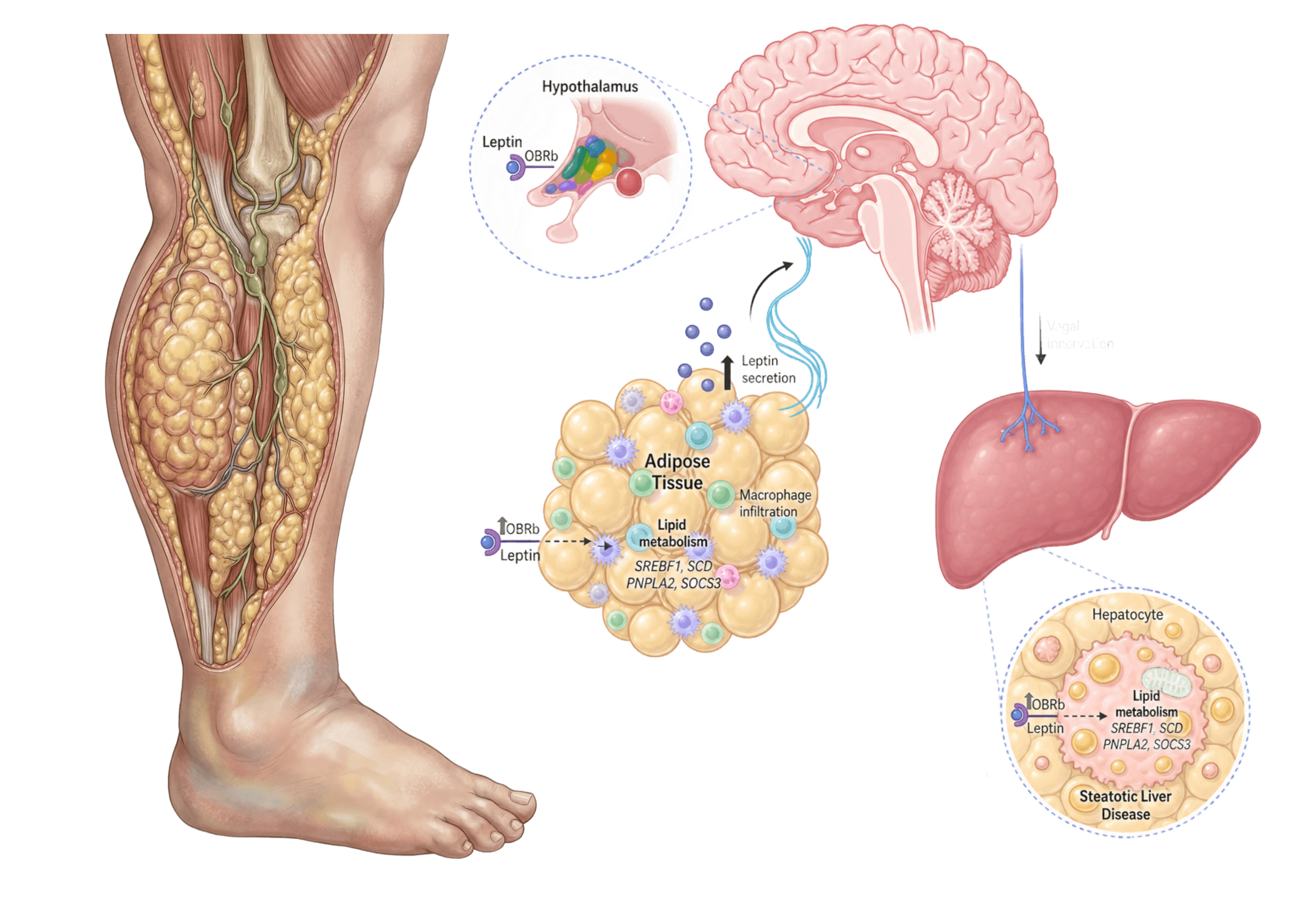
Leptin, Scarcity Signals and the Female Brain
Leptin illustrates this principle particularly well. Leptin is often described superficially as a satiety hormone, but its role is much broader. It functions as an endocrine signal communicating information about energy status to the brain. Women with functional hypothalamic amenorrhea frequently show lower leptin levels than eumenorrheic controls, even when researchers adjust for body composition. This suggests that the reproductive axis responds not simply to absolute fat mass, but to the body’s interpretation of energetic sufficiency.
This becomes deeply relevant when discussing women who appear “healthy” externally yet experience disrupted cycles, infertility or hormonal suppression after prolonged periods of underfueling, psychological stress or overtraining. The female reproductive system is remarkably sensitive to signals suggesting scarcity or physiological threat.

Importantly, leptin is not the entire explanation. Modern research points toward a complex interaction involving kisspeptin neurons, GnRH signaling, cortisol regulation, thyroid function, inflammatory mediators and psychological stress pathways. While small interventional studies using recombinant leptin demonstrated partial restoration of reproductive function in some women with hypothalamic amenorrhea, this should not be misunderstood as established routine clinical treatment. Current guidelines from Endocrine Society still emphasize restoration of adequate nutrition, reduction of physiological and psychological stressors and normalization of energy balance as the primary intervention.
Stress Is Also a Hormonal Signal
Stress itself remains profoundly underappreciated in discussions about female hormones. Functional hypothalamic amenorrhea is not simply a disorder of thinness or calorie restriction. Many women with FHA also demonstrate elevated cortisol levels, increased anxiety, disturbed sleep, perfectionistic traits or disordered eating patterns. Psychological stress and metabolic stress interact continuously within the neuroendocrine system.
For women with lipedema, this perspective may feel unexpectedly validating. Living with chronic pain, swelling, body image distress, repeated medical dismissal and constant pressure to lose weight creates a significant physiological burden. The body does not separate emotional stress from biological stress as neatly as wellness culture often implies. Chronic stress signaling can influence inflammation, appetite regulation, sleep quality, insulin sensitivity and reproductive hormone signaling simultaneously.


When Excess Adiposity Also Becomes a Hormonal Stressor
At the other end of the spectrum, excessive adiposity can also disrupt reproductive physiology, particularly when visceral or central adiposity becomes metabolically dominant. Research summarized by American Society for Reproductive Medicine demonstrates associations between obesity, ovulatory dysfunction, menstrual irregularities and subfertility. Yet even here, simplistic explanations fail. The issue is rarely “too much estrogen” alone. Instead, researchers increasingly focus on the interaction between insulin resistance, chronic low-grade inflammation, altered adipokine signaling, hyperandrogenism, reduced SHBG production and ovarian dysfunction.
This is another reason why body composition alone cannot fully explain hormonal health.
Two women with similar BMI values may have profoundly different endocrine profiles depending on fat distribution, inflammatory state, insulin sensitivity, stress burden, sleep quality, genetics and overall metabolic function. Visceral fat appears metabolically more disruptive than subcutaneous gluteofemoral fat in many contexts, and adipose tissue itself behaves differently depending on anatomical location. This complexity becomes highly relevant in lipedema because lipedema adipose tissue appears biologically distinct from ordinary obesity in several important ways, including inflammatory signaling, vascular alterations and pain mechanisms.
The Problem With Simplistic Diet Culture
The discussion around dietary fat also deserves far more nuance than most women were taught growing up. The scientific literature does not support the idea that eating dietary fat automatically improves hormones in a simplistic way, nor does it support decades of extreme low-fat ideology. What matters far more is the broader physiological environment in which the body operates. A woman consuming low-fat products while chronically underfueling, sleeping poorly, overtraining and experiencing persistent stress may place the reproductive axis under substantially greater strain than someone eating a balanced diet with adequate energy availability and metabolic stability.
Similarly, high-fat diets themselves are not magical hormonal cures. Modern guidelines for conditions such as PCOS increasingly emphasize overall dietary quality, sustainability, insulin sensitivity and lifestyle patterns rather than rigid macronutrient dogma. The body responds to integrated signals, not isolated nutrition slogans.
Hormones Do Not Simply “Float Around in Fat”
Another commonly misunderstood aspect involves hormone transport. Sex hormones do not circulate primarily through “fat in the blood.” Instead, hormones such as estradiol and testosterone are largely transported bound to proteins such as sex hormone-binding globulin and albumin. SHBG itself is highly sensitive to metabolic status. Insulin resistance and obesity often suppress SHBG production, increasing free androgen exposure and altering hormonal balance. This is one reason why metabolic dysfunction can influence reproductive physiology even when absolute hormone concentrations do not appear dramatically abnormal.
What Women With Lipedema Deserve to Understand
For women with lipedema, the most important takeaway may not be a specific diet rule or hormone theory, but a different conceptual understanding of the female body itself.
Female endocrinology is deeply energy-sensitive, stress-sensitive and metabolically interconnected. Adipose tissue is biologically active. Hormonal health cannot be reduced to simplistic statements about calories, fat grams or body weight alone. The body continuously interprets information about safety, nourishment, inflammation, recovery and energetic sufficiency.
And perhaps this explains why so many women with lipedema feel misunderstood by conventional health narratives. Many were taught to view their bodies through an overly simplistic framework where body fat was treated merely as stored excess to be eliminated. But modern research increasingly shows that adipose tissue participates in endocrine signaling, immune regulation and metabolic communication in ways far more sophisticated than older models suggested.
Understanding this complexity does not mean abandoning metabolic health or pretending nutrition no longer matters. It means moving beyond reductionist explanations that fail to capture the biology women are actually living inside.
If this article challenged something you previously believed about hormones, fat tissue or lipedema, I would genuinely like to hear your thoughts.
What is one thing about female metabolism or hormonal health that nobody ever properly explained to you before?
Functional Hypothalamic Amenorrhea: An Endocrine Society Clinical Practice Guideline (DOI: 10.1210/jc.2017-00131)
Current understanding of hypothalamic amenorrhoea (DOI: 10.1177/2042018820945854)
Where Have the Periods Gone? The Evaluation and Management of Functional Hypothalamic Amenorrhea (DOI: 10.4274/jcrpe.galenos.2019.2019.S0178)
Functional hypothalamic amenorrhea: Impact on bone and neuropsychiatric outcomes (DOI: 10.3389/fendo.2022.953180)
Low energy availability, not exercise stress, suppresses the diurnal rhythm of leptin in healthy young women (DOI: 10.1152/ajpendo.2000.278.1.E43)
Energy availability discriminates clinical menstrual status in exercising women (DOI: 10.1186/s12970-015-0072-0)
Energy Availability Is Associated With Luteinizing Hormone Pulse Frequency and Induction of Luteal Phase Defects (DOI: 10.1210/clinem/dgz030)
Leptin in human physiology and pathophysiology (DOI: 10.1152/ajpendo.00315.2011)
Leptin signaling and circuits in puberty and fertility (DOI: not retrieved)
Gender differences in the regulation of P450 aromatase expression and activity in human adipose tissue (DOI: 10.1038/0801254)
Glucocorticoid regulation of P450 aromatase activity in human adipose tissue: gender and site differences (DOI: 10.1210/jcem.87.3.8288)
The Intimate Relationship between Adipose Tissue, Fertility, and Bone (DOI: 10.22540/JFSF-11-080)
The Impact of the Endocrine and Immunological Function of Adipose Tissue on Reproduction in Women with Obesity (DOI: 10.3390/ijms25179391)
Obesity and risk of female reproductive conditions: A Mendelian randomisation study (DOI: 10.1371/journal.pmed.1003679)
Higher waist circumference is associated with increased likelihood of female infertility: NHANES 2017–2020 results (DOI: 10.3389/fendo.2023.1216413)
IOC consensus statement on relative energy deficiency in sport (RED‑S): 2018 update (DOI: 10.1136/bjsports-2018-099193)
2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) (DOI: 10.1136/bjsports-2023-106994)
Does Relative Energy Deficiency in Sport (REDs) Syndrome Exist? (DOI: 10.1007/s40279-024-02108-y)
Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome (Hum Reprod) (DOI: 10.1093/humrep/dead156)