
The Truth About Carbohydrates, Water Retention, and Lipedema

If you live with lipedema, you may know this feeling well. You wake up after a day where you ate a little differently than usual, maybe more bread, more rice, dessert, sushi, pizza, or simply more carbohydrates than your body is used to, and the next morning the scale is suddenly up by one or two kilos. Your legs feel tighter. Your skin feels more tender. Your rings may fit differently. Your body feels puffy, heavy, and inflamed. And even if you understand nutrition, there is often still a moment of panic.

Did I gain fat overnight?
Did I ruin my progress?
Is my lipedema getting worse?
For many women with lipedema, these moments can become emotionally loaded. The body already feels unpredictable. The tissue can already feel painful, heavy, and unresponsive. So when the scale jumps quickly, it is easy to assume the worst.
But in many cases, what you are seeing is not sudden fat gain. It is fluid.
And understanding that difference can change not only how you interpret your body, but also how you care for it.

This is one of the most important things women with lipedema need to know. Weight does not always mean fat. Swelling does not always mean failure. And a day with more carbohydrates does not mean your body has suddenly moved backwards in any meaningful or permanent way.
At the same time, lipedema is not “just water” either. This is where things become more nuanced. Because while glycogen related water retention is a normal physiological process in all humans, women with lipedema often experience it more intensely. The body is not simply storing carbohydrate in muscles and liver. It is doing so in the context of altered fat tissue, increased tenderness, inflammatory signaling, and tissue that is already prone to fluid accumulation.
To understand why one high carb day can feel so dramatic, we first need to understand what normally happens in the body when you eat carbohydrates.

The normal physiology of carbohydrates, glycogen, and water
Carbohydrates are not inherently bad. They are one of the body’s main fuel sources. After you eat carbohydrate containing foods, they are broken down into glucose and absorbed into the bloodstream. The body then uses some of that glucose immediately for energy, especially in tissues like the brain, muscles, and other organs with high energy demands.
What the body does not use right away can be stored.
The primary storage form of carbohydrate is glycogen. Glycogen is stored mainly in the liver and muscles. It acts as a reserve that your body can draw on later, especially between meals, during exercise, or during periods of fasting.
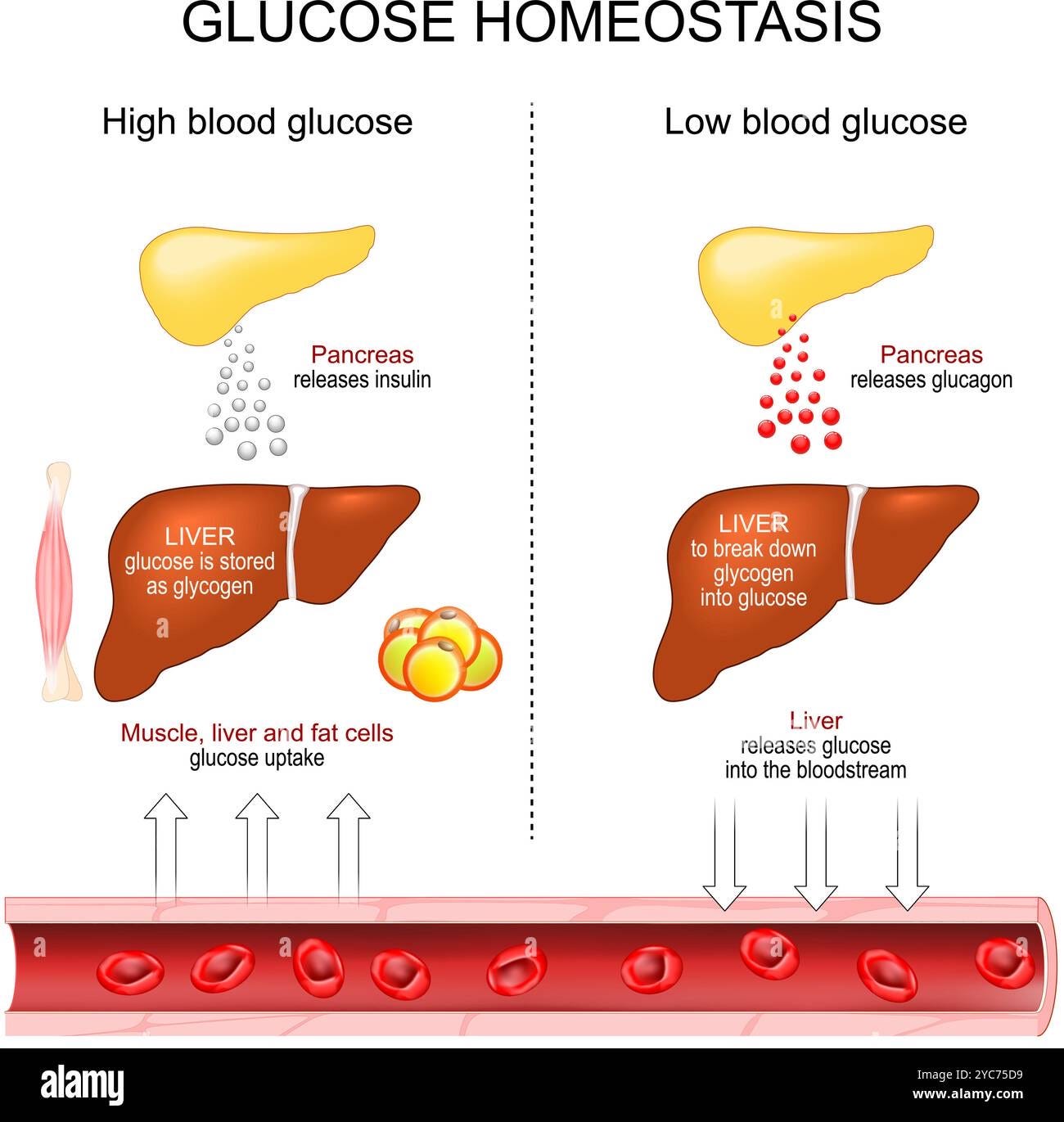
Here is the part many people never learn clearly. Glycogen is stored together with water. For every gram of glycogen, the body binds several grams of water. The exact number varies across textbooks and study contexts, but the common rule of thumb is that one gram of glycogen is stored with roughly three grams of water.
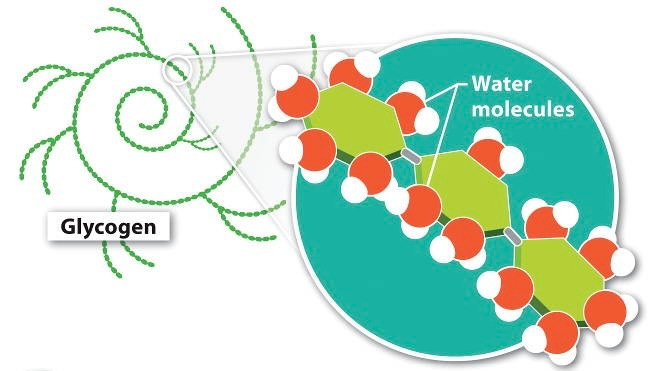
This means that when glycogen stores increase, body weight can rise quickly, even when body fat has not changed at all.
This is why athletes often gain weight when they increase carbohydrate loading before competition. It is why people starting a low carbohydrate diet often lose weight rapidly in the first days, even before significant fat loss has occurred. And it is why one day of higher carbohydrate intake can make the scale jump the next morning.
This is not mysterious. It is not abnormal. It is basic physiology.
In a person without lipedema, this may show up as mild puffiness, a fuller look, or a temporary increase on the scale. In someone with lipedema, the same physiological shift can feel much more dramatic.
Why lipedema changes the picture
Lipedema is not simply a problem of “fat that won’t go away.” It is a chronic connective and adipose tissue disorder with characteristic changes in subcutaneous fat, tissue architecture, pain, and fluid handling. The fat tissue is different from typical fat tissue. The microenvironment is different. The way the tissue behaves under pressure is different.
In lipedema, the tissue is often marked by enlarged fat cells, altered extracellular matrix, increased fibrosis, and signs of vascular dysfunction. Small vessels in the affected tissue may be more fragile or more permeable than normal. Inflammatory cells and inflammatory mediators are often more active. Interstitial fluid can accumulate more easily, and the tissue can feel swollen, pressured, and tender even when the swelling is not the same as classic lymphedema.

This distinction matters.
Women with lipedema often describe swelling in a way that does not fit neatly into traditional categories. It may not be classic lymphatic swelling at first. It may be more of an interstitial fluid burden, a vascular leak phenomenon, a tissue congestion problem, or a pain pressure phenomenon driven by abnormal fat and connective tissue. Whatever language one prefers, the lived experience is familiar. The tissue can hold onto fluid more readily and react more intensely.
So when glycogen stores rise after a higher carbohydrate day and bring additional water with them, that water is entering a body that may already be more vulnerable to fluid related discomfort. That is why what is a mild shift for one person may feel like a major flare for a woman with lipedema.
This is not because carbohydrates are evil. It is because lipedema changes the terrain.
Why the scale can jump by one to two kilos overnight
Let us make this practical.
If you normally eat in a lower carbohydrate range and then have a day with significantly more carbohydrates, perhaps through restaurant food, dessert, bread, pasta, fruit, or simply larger portions, your body may replenish glycogen stores. As glycogen increases, water comes with it. Sodium intake is often higher on these days too, especially if the food is processed, restaurant based, or more indulgent than your usual meals. Sodium further encourages water retention. Hormonal status can amplify this again, particularly in the luteal phase of the cycle or during periods of stress.
Now add lipedema to that picture.

Instead of just seeing a harmless jump on the scale, you may also feel:
heavier legs
more tenderness
more pressure in the calves or thighs
greater sensitivity to touch
more visible swelling in arms or legs
less comfort in compression garments
a sense of being inflamed or “off”
This can be very distressing, especially if you are trying to take care of your condition carefully. But it is essential to remember that fat gain does not happen at this speed.
To gain a meaningful amount of body fat overnight, you would need a large sustained energy surplus, far larger than what most women imagine after one dinner or one social day. A rapid increase from one day to the next is far more likely to reflect shifts in glycogen, sodium, gut content, hormones, and fluid rather than actual adipose tissue growth.
For women with lipedema, that fluid shift can still be painful and significant. But it is not the same as suddenly gaining one or two kilos of fat.
Why this matters psychologically
This knowledge is not only physiologically important. It is emotionally protective.
Many women with lipedema have a history of trying very hard and feeling like the body does not respond in proportion to their efforts. They may have experienced diets that worked on paper but not in the tissue they most desperately wanted to change. They may have felt dismissed by health professionals who reduced everything to overeating. They may have internalized shame around weight, swelling, or body shape.

In that context, a sudden rise on the scale can trigger fear, guilt, or a powerful urge to overcorrect.
This is where problems often begin.
One swollen morning can lead to panic restriction. Panic restriction can lead to rebound eating, more stress, poorer recovery, increased inflammation, and a worsening relationship with food. The body becomes something to control rather than something to understand.
A science based approach helps interrupt that cycle. It allows you to say this is a fluid shift. My body is reacting. I need to support it, not punish it.
That is a profoundly different mindset.
Does this mean women with lipedema should avoid carbohydrates completely
No. Not necessarily.
This is where the conversation needs maturity.

Some women with lipedema genuinely feel much better on lower carbohydrate or ketogenic diets. They may notice less swelling, less pain, less fluctuation, and more predictable energy. For them, keeping carbohydrate intake lower and more stable may be one of the most helpful symptom management tools they have.
Other women do not want to eat that way, cannot sustain it, or simply feel better with a more mixed diet that includes carbohydrates. They may enjoy oats, berries, legumes, potatoes, quinoa, fruit, or rice and still manage their lipedema well when their overall diet is structured, minimally processed, and metabolically supportive.
Both of these women can take good care of themselves.
The goal of a thoughtful lipedema approach is not to push one rigid dietary identity. It is to understand what different foods do in your own body, and to build a pattern that reduces suffering while remaining sustainable.
A woman who feels best low carb should not be told she must eat more carbohydrate to be “balanced.” A woman who includes carbohydrates thoughtfully should not be told she is sabotaging herself by default.
This is not about ideology. It is about biology, symptom patterns, lifestyle, and long term adherence.
What carbohydrates actually do in lipedema
It helps to separate three different questions.
First, do carbohydrates automatically worsen lipedema pathology in every woman. Not necessarily.
Second, can higher carbohydrate intake increase water retention and make symptoms temporarily worse in many women with lipedema. Yes, that is very plausible and commonly experienced.
Third, does the type, amount, timing, and context of carbohydrate intake matter. Absolutely.

The body does not respond the same way to a large evening meal of refined carbohydrates, alcohol, salty restaurant food, and dessert as it does to a balanced lunch with quinoa, salmon, vegetables, and olive oil. Fiber changes the speed of absorption. Protein changes the insulin response. Movement changes glycogen use. Portion size matters. Sleep matters. Menstrual timing matters. Total diet quality matters.
This is why the carbohydrate conversation should never be reduced to a simplistic yes or no.
If you eat carbohydrates, how to do it more wisely
For women with lipedema who want to include carbohydrates, the most helpful strategy is usually not to chase perfection, but to aim for steadiness.

Large swings often create the biggest symptom swings. Very low one day and very high the next can make the body feel more unstable, especially if those higher carb days are also high in sodium and low in fiber.
It is often more helpful to:
choose slower digesting carbohydrate sources
combine carbohydrates with protein, fat, and fiber
avoid building meals around refined carbohydrates alone
be mindful of portion size
notice whether timing affects your swelling
expect some fluctuation without catastrophizing it
Complex, fiber rich carbohydrate sources often sit better in a lipedema sensitive body than highly processed ones. Berries, legumes, oats, quinoa, buckwheat, vegetables, and moderate portions of starchy foods combined with protein and healthy fats will often behave very differently from pastries, white bread, sugar heavy snacks, sweetened drinks, or ultra processed convenience foods.

This does not mean never eat those foods. It means understand their likely effect.
If you know you swell more after a restaurant meal, that knowledge can help you plan. Maybe you wear compression more deliberately the next day. Maybe you hydrate better. Maybe you go for a walk after the meal. Maybe you simply remind yourself this is temporary.
That is very different from feeling blindsided.
If you do better on lower carb, that can be valid too
For many women with lipedema, lower carbohydrate eating reduces symptom noise.
With fewer glycogen fluctuations, there is often less associated water fluctuation. Appetite may feel steadier. The body may feel less puffy. Pain may improve. Energy can feel more stable, especially when the diet is built around adequate protein, healthy fats, and micronutrient rich whole foods.
This can be an extremely useful tool.
But even here, quality matters. A lower carbohydrate diet is not automatically anti inflammatory simply because it is low in carbs. A diet built on processed meats, poor quality fats, and chronic undereating is not the same as a nutrient dense lower carb pattern that includes fish, eggs, olive oil, avocado, vegetables, herbs, and sufficient total energy.
Low carb is not magic. It is one possible way of reducing fluctuations and improving symptom control.
For some women it is life changing. For others it is too restrictive or unnecessary. The point is not to create hierarchy. The point is to respect variability.
Why fiber still matters
One of the easiest mistakes in the lipedema world is to make the conversation so carbohydrate focused that fiber gets forgotten.
Fiber matters, whether you eat lower carb or moderate carb.
It helps with satiety, supports bowel regularity, improves post meal glucose control, and supports the gut microbiome. A healthier microbial environment can influence inflammatory tone, and anything that improves metabolic steadiness tends to be helpful in a condition where tissue sensitivity and low grade inflammation are already present.
Many lower carbohydrate approaches can still be fiber rich if they are built around vegetables, seeds, nuts in appropriate portions, berries, and other minimally processed plant foods. Many moderate carbohydrate approaches can also be fiber rich if the carbohydrates chosen are intact, slowly digested, and not dominated by refined starches and sugar.
The real divide is not simply carb versus no carb. It is more often structured whole food eating versus chaotic symptom provoking eating.
Why inflammation and fluid are so connected in lipedema
Lipedema is often described through the lens of fat, but the lived condition is as much about fluid and pressure as it is about adipose tissue itself.
Women do not just describe size. They describe bursting, aching, tenderness, heaviness, bruising, and a feeling that the tissue is under internal strain.
This is one reason why even temporary water retention can feel so severe. Additional fluid in a healthy tissue compartment is not experienced the same way as additional fluid in tissue that is already fibrotic, pressure sensitive, and structurally altered.
The tissue environment matters.
Inflammation can increase vascular permeability. Altered vasculature can encourage more fluid escape into the tissue. Fibrosis can impair normal fluid movement. Pain signaling may become amplified. So a relatively small dietary or hormonal trigger can create a disproportionate symptom response.
This is also why symptom management in lipedema usually cannot rely on food alone.
The role of conservative therapies
Diet matters, but lipedema care is broader than diet.
Conservative therapies exist because the problem is not purely nutritional. It is mechanical, vascular, inflammatory, connective, and often neurological in how it is experienced.
Compression can help limit fluid accumulation and support tissue comfort. Manual therapies may help some women with drainage and symptom relief. Movement, especially low impact movement, can support circulation and function. Strength training helps preserve lean mass and supports overall metabolic health. Skin care matters. Recovery matters. Managing long periods of standing or sitting matters.
For many women, the best results come from combining approaches rather than searching for one perfect solution.
A woman who eats well but never supports her tissue mechanically may still struggle. A woman who uses compression but lives on foods that repeatedly trigger large symptom swings may still struggle. A woman who pursues only weight loss without muscle preservation may become lighter but not necessarily more resilient.
This is why lipedema management is best understood as layered care.
Why not every flare means progression
One of the most important things to understand is that a flare is not always the same as disease progression.
Progression is a long term pattern of worsening. It may involve increasing tissue burden, more fibrosis, greater symptoms, reduced function, or evolving complications over time.
A flare is a short term worsening. It may be triggered by carbohydrates, sodium, hormonal changes, travel, heat, sleep disruption, stress, illness, prolonged standing, intense exercise, or inflammatory foods. It can feel dramatic without representing permanent change.
Many women confuse the two because flares feel so real. The legs genuinely feel worse. The body genuinely looks different. Pain genuinely increases.
But the fact that it is real does not mean it is permanent.
Learning to tell the difference can be deeply calming. It allows for response instead of fear.
How to respond after a high carb or high swelling day
The best response is usually not punishment. It is re regulation.
Return to your normal structure. Hydrate. Prioritize whole foods. Use compression if it helps you. Move gently. Eat protein. Reduce chaos. Sleep. Let your body settle.
You do not need to starve the next day. You do not need to “earn back” a meal. You do not need to panic fast unless fasting is already part of a pattern that genuinely works for you and does not dysregulate you.
In most cases, the body will normalize when routine normalizes.
This is where trust becomes important. Women with lipedema often feel they cannot trust their bodies because the tissue behaves unpredictably. But over time, you can learn to trust the patterns even if you do not always like them.
You can learn this meal made me swell. This part is fluid. This is my luteal phase. This is travel swelling. This is sodium. This is a real flare. This is not body fat appearing overnight.
That kind of body literacy is powerful.
What to track instead of obsessing over the scale
For women with lipedema, the scale can be a blunt instrument.
It is not useless. But it is incomplete.
A better picture often comes from combining body weight with other markers such as:
how your legs feel
how your compression fits
waist to limb difference over time
weekly or monthly circumference measurements
pain levels
energy
mobility
sleep
menstrual phase
what you ate the day before
whether you traveled, stood a lot, or slept poorly
This creates context. Context is what protects you from misinterpreting normal variation as failure.

It also helps you personalize your approach. Some women learn they tolerate moderate carbohydrates very well when they are paired with protein and eaten earlier in the day. Others realize certain foods consistently trigger swelling regardless of the carbohydrate number itself. Some discover that sleep deprivation is a bigger flare driver than fruit or oats ever were.
This is why observation matters more than dogma.
The bigger truth about food and lipedema
Women with lipedema often get pulled into extremes.
One extreme says calories are all that matters. That is too simplistic.
The other says calories do not matter at all, and only hormones, inflammation, or disease mechanisms count. That is also incomplete.
The more honest truth sits in the middle.
Lipedema is a disease of altered tissue biology. It is not caused by a lack of discipline. It does not behave exactly like ordinary weight gain. It involves fluid, inflammation, pain, connective tissue changes, and likely deeper metabolic and vascular features that are still being clarified.
And still, nutrition matters.
Water balance matters. Glycogen matters. Insulin dynamics matter. Fiber matters. Food quality matters. Energy balance matters. The mechanical burden of more tissue matters. The inflammatory burden of ultra processed eating matters.

These things are not the whole story. But they are very much part of the story.
A gentler and smarter framework
Instead of asking do I need to stop eating carbohydrates, a more helpful question may be what kind of eating pattern helps my body feel most stable.
Instead of asking why did I gain two kilos overnight, a better question may be what changed in my fluid, glycogen, sodium, hormones, or inflammation.
Instead of asking what diet is best for lipedema, perhaps the more useful question is what way of eating reduces my symptoms, protects my muscle, supports my quality of life, and remains sustainable over years.
For some women, that will be lower carb. For others, that will be a Mediterranean style pattern with moderate carbohydrates and strong attention to food quality. For others, it may be a hybrid approach with generally stable eating and thoughtful flexibility.
There is room for all of these women in the lipedema conversation.
The conclusion women with lipedema need to hear
Yes, a higher carbohydrate day can make you weigh more the next morning.
Yes, much of that is likely water bound to glycogen, along with sodium related fluid retention and general tissue congestion.
Yes, lipedema can make this feel much worse than it does in bodies without altered fat tissue and fluid sensitivity.
But no, this does not usually mean you gained body fat overnight.
And no, it does not mean you failed.
The body with lipedema is often more reactive, more pressure sensitive, and more vulnerable to fluid related discomfort. That means you may need more strategy, more observation, and more support. It does not mean you need more shame.
The goal is not to fear food. The goal is to understand how your body responds to it.

The goal is not to force yourself into a dietary identity that does not fit you. The goal is to find the pattern that gives you the most stability, the least suffering, and the greatest sustainability.
And perhaps most importantly, the goal is to stop mistaking temporary fluid shifts for permanent damage.
Because when you understand what your body is doing, you can stop fighting it in panic and start supporting it with precision.
Most of the photos I have are from the 20% of my life where I’m truly enjoying myself. I’ll try to share more from the other 80% as well, so you can see what that part really looks like.
My body does tend to jump in weight with carbs such as bread, cake, pasta, rice. Found this very interesting. Thank you.