
Something Strange Is Happening Inside Lipedema Fat Cells
A microscopy study published weeks ago found a structural signature inside lipedema fat cells, previously linked to something very different from ordinary fat, with images unlike anything I have seen.

There is a particular kind of exhaustion that comes from being told, over and over again, that your tissue is simply fat. That the heaviness in your legs is a lifestyle problem. That the pain, the bruising, the nodules pressing beneath your skin, the relentless resistance to all the things that are supposed to work — that all of it can be explained by ordinary fat biology. Many of us with lipedema have spent years in that space, caught between what our bodies are clearly telling us and what the medical system has been willing to acknowledge. What we have needed, and what research has been slowly — sometimes frustratingly slowly — beginning to provide, is a more serious biological account of what is actually happening in this tissue.
A study published just a few weeks ago gives us something I did not expect to find in 2026: a completely new way of looking at lipedema, quite literally. Not at the whole tissue, not at inflammatory markers in the blood, not at lymphatic architecture or connective tissue changes — but at something much smaller and, in some ways, much more fundamental. The researchers looked inside the fat cells themselves. And what they found there, under very high magnification, is something that raises questions about lipedema biology that I do not think anyone has properly asked before.
The following section is for subscribers of LipedemaScience. Become a subscriber today.
Why? Because this is where you’ll find lipedema research explained in language you can actually understand, and it is also a place where you can ask questions.
I have worked in the lab for years, with cells, peptides, DNA, and inflammation markers such as cytokines. I have also published scientific articles in peer-reviewed journals related to food science.
The paper I am talking about is “Adipocytes from lipedema adipose tissue show lipoma-associated nuclear atypia”, published on May 1st, 2026, in Frontiers in Cell and Developmental Biology by Steiner, Rinnerthaler, Mueller, Russe, Lipp and Bauer from the University of Salzburg, Austria. The Salzburg group has been doing serious, technically demanding work on lipedema tissue for several years now, and this study is perhaps their most morphologically striking contribution yet.
Let me tell you what they did and what they found — carefully, because the terminology can sound alarming if pulled out of context, and this is not an alarming finding. It is a fascinating one.
Help grow this community by sharing the article with someone you care about who might find this fascinating.
Looking inside lipedema fat cells — at the nucleus
The researchers used two forms of microscopy: light microscopy and transmission electron microscopy, the latter being an extraordinarily high-resolution technique that can visualize structures at the nanometer scale — far below what conventional clinical microscopy can reach. They analyzed approximately 3,000 adipocyte cross-sections from subcutaneous adipose tissue samples: nine from women with lipedema and five from non-lipedema controls. All donors were non-obese. Tissue was collected from the extremities — upper arms and lateral thighs — specifically from the deeper subcutaneous layer, during liposuction procedures.
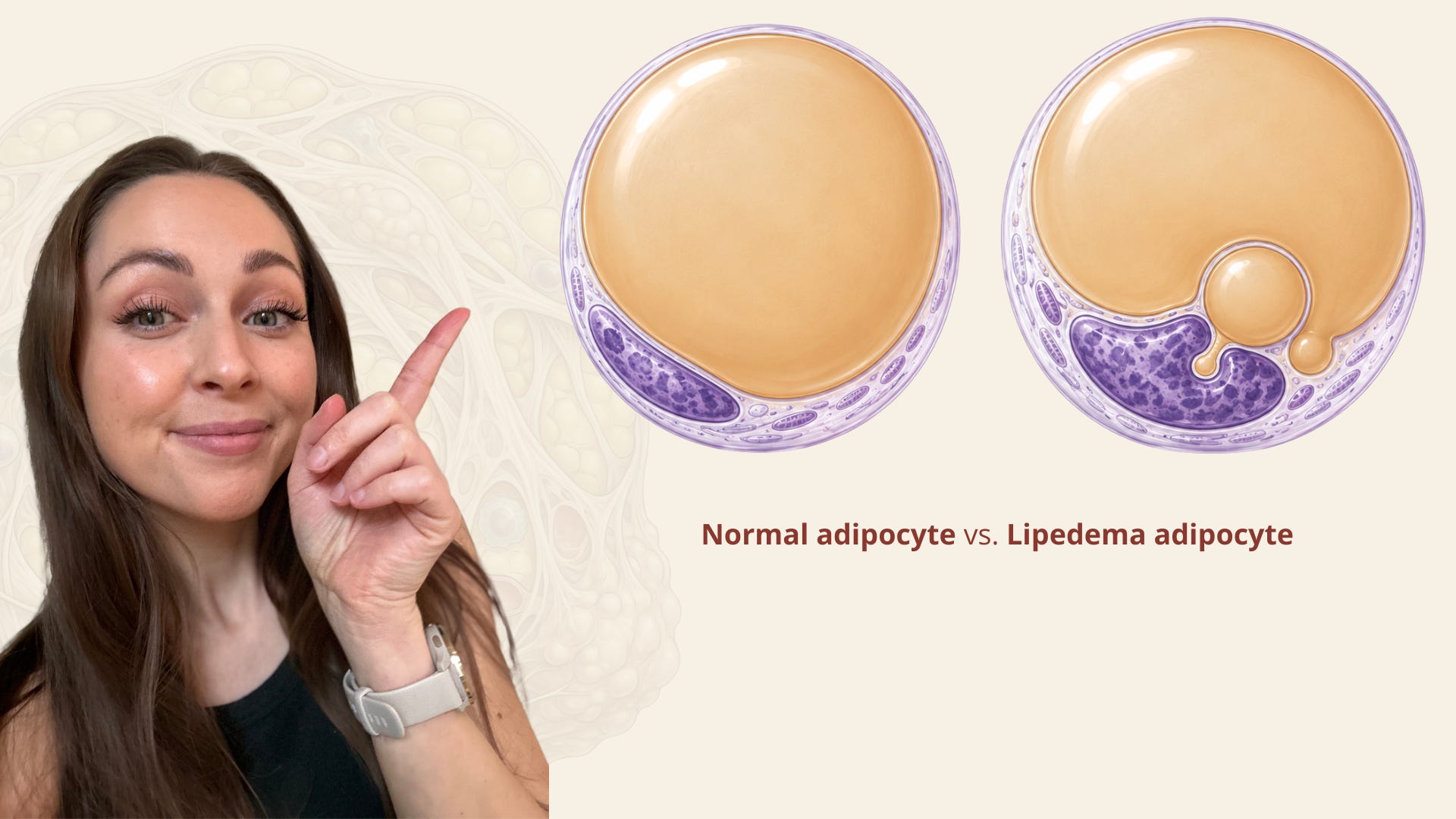
What they were looking for — and what they found — is a structural feature of adipocyte nuclei called a Lochkern.
The word is German, and it means something close to “nucleus with a hole.” It describes a fat cell nucleus that has been deformed — indented, pushed inward, distorted in shape — so that in cross-section it appears to contain a hole or a notch or a ring-like space. Different morphological forms have been described in the older histological literature under names like Ringkerne (ring nuclei) and Kerbenkerne (notch nuclei), but the researchers use Lochkerne here as a single umbrella term for all varieties of nuclear indentation.
Before you read the result, you need to know one thing about these nuclear structures: they are not normally found in ordinary adipose tissue in meaningful numbers. They are associated primarily with lipomas — the benign fatty growths that occur in various lipomatous conditions. Finding them in normal fat is unusual. Finding them frequently is even more so.
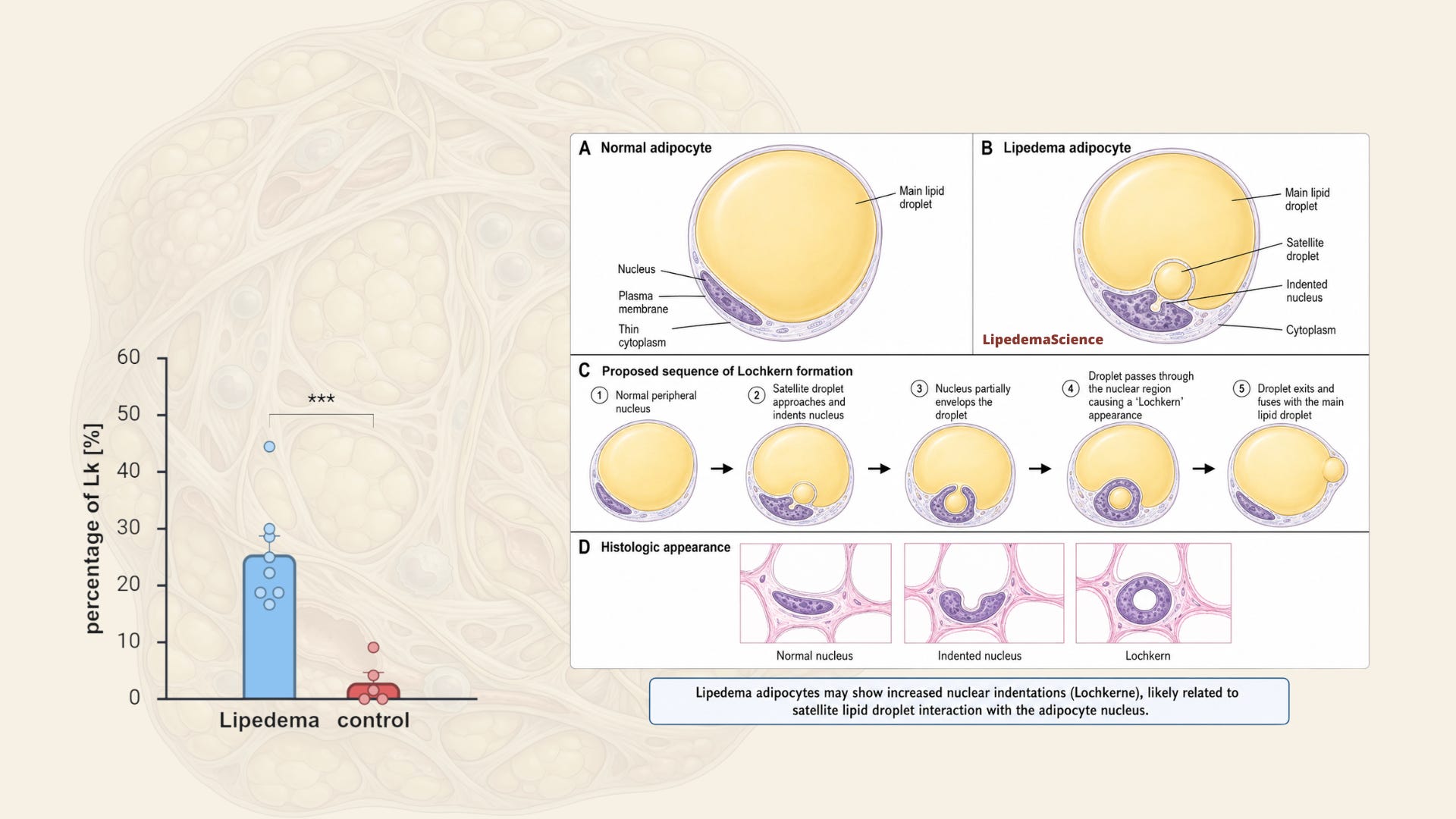
In the lipedema samples, 24% of identifiable adipocyte nuclei showed Lochkerne. In the control samples, that number was 3%. The difference was statistically significant at p = 0.001. And when the researchers checked whether this difference could simply be explained by the slightly different average BMI or age between the groups, they found no such relationship — Lochkern frequency did not correlate with either variable in their dataset.

What Lochkerne actually are — and how they form
This is where I want to slow down, because the electron microscopy images in this paper are genuinely unlike anything I have seen in lipedema research before. They do not just document the presence of Lochkerne — they show their formation in real tissue, step by step.
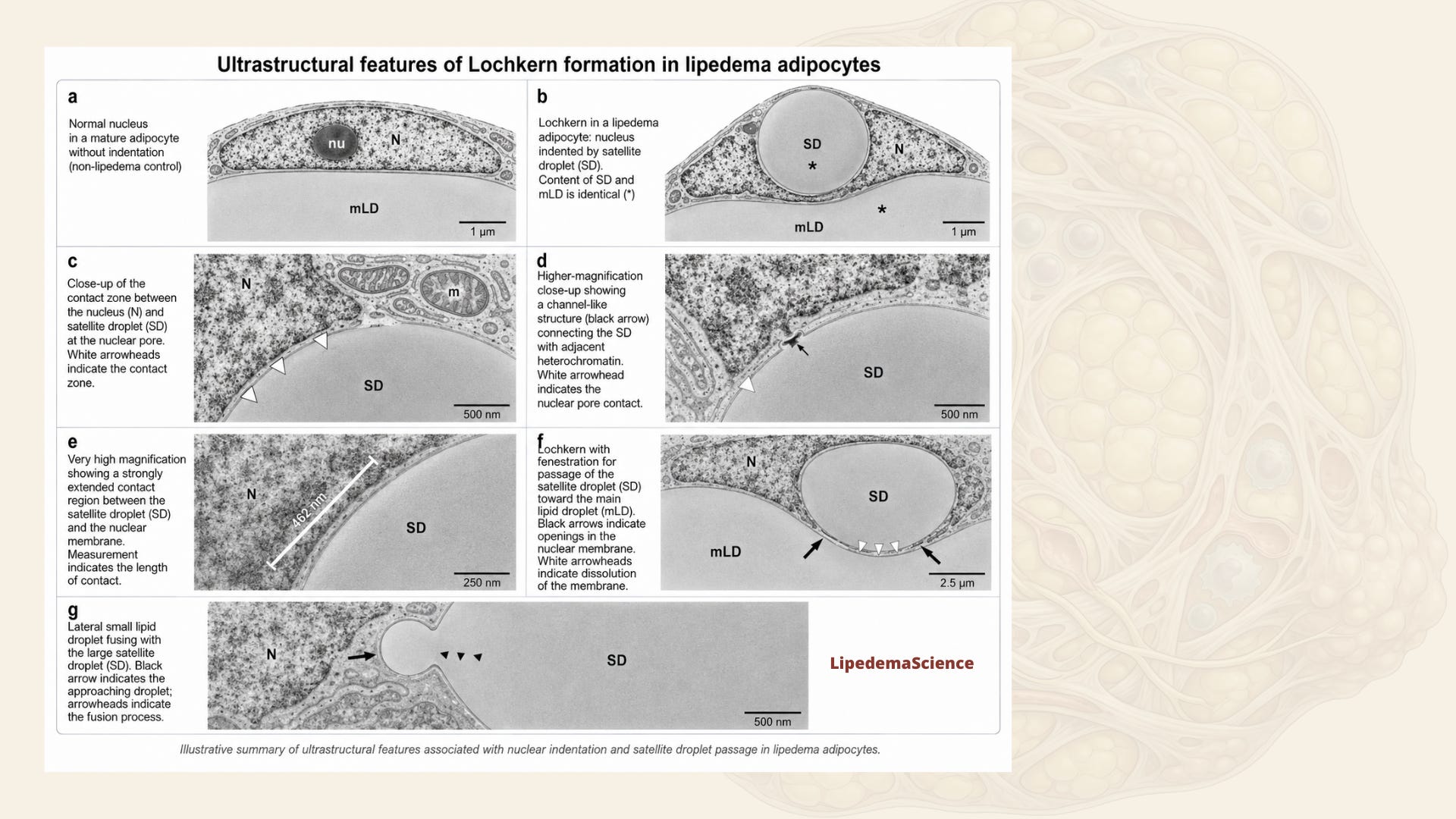
In paraffin histology — the standard technique used in most clinical settings — lipids are dissolved away during tissue processing. This is why Lochkerne have historically looked like empty holes: the lipid that created the indentation is simply gone by the time you look at the slide. With transmission electron microscopy and epoxy resin embedding, lipids are chemically fixed and preserved by osmium tetroxide. This means you can see them exactly where they were in the living tissue. And what this reveals changes the picture entirely.
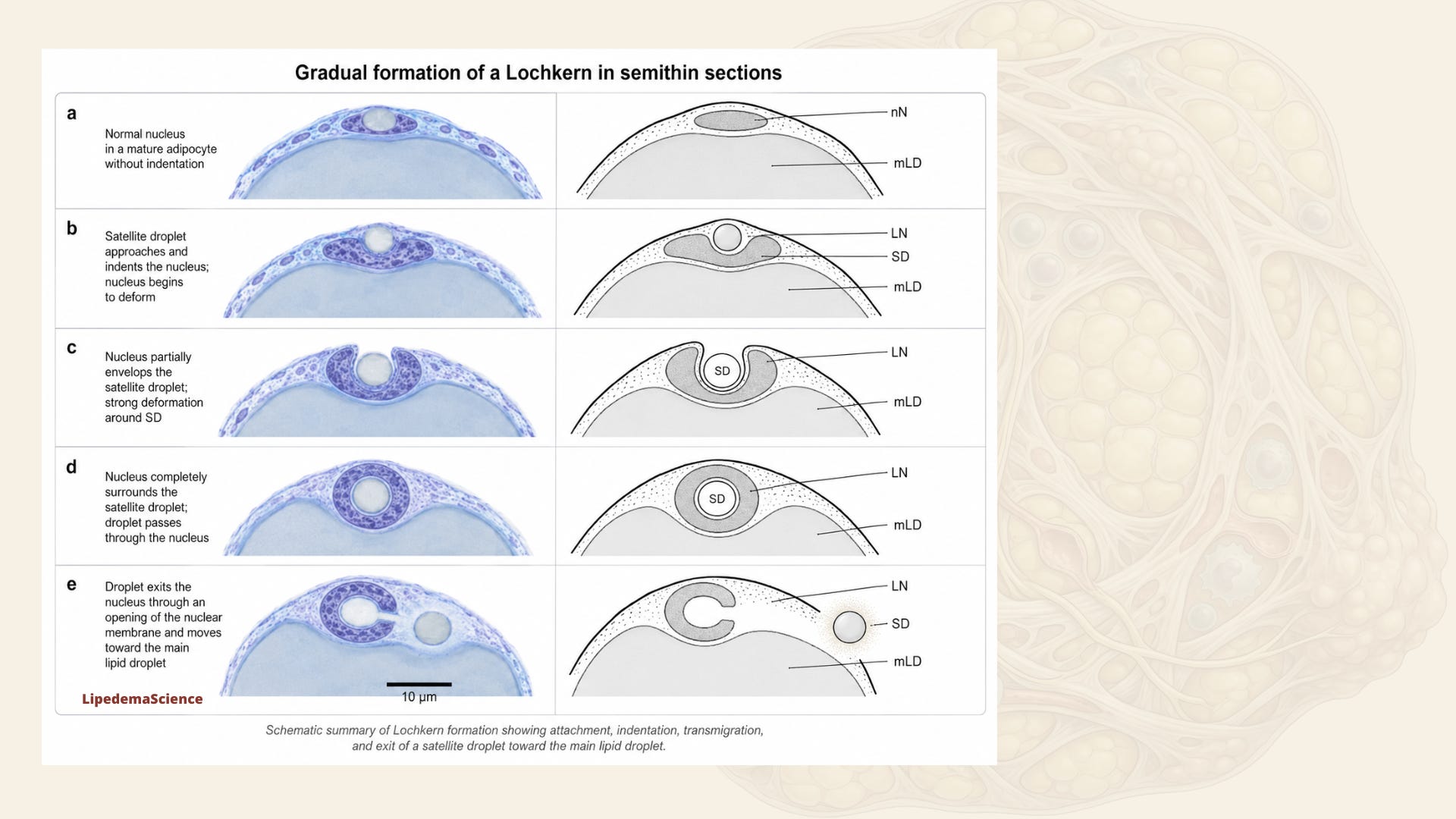
The researchers describe — and document through a beautifully constructed sequence of images — the involvement of what they call satellite droplets: small lipid droplets that form in the narrow cytoplasmic space between the nucleus and the plasma membrane of the fat cell, arising from the endoplasmic reticulum. In the Salzburg images, you can follow what appears to be a progression: a satellite droplet approaches the nucleus, makes contact with the nuclear membrane, begins to press into it. The nucleus deforms visibly around the droplet — it bulges, it contorts. The droplet then appears to move through the nuclear region, with the nuclear membrane opening around it, until it exits on the other side and fuses with the large central lipid droplet that occupies most of the mature fat cell.
This sequence — approach, indentation, transmigration, fusion — is what creates the Lochkern appearance. The paper includes a figure that pairs microscopy images with schematic drawings of each stage, and the result is unusually clear for a study of this technical complexity. The electron micrographs show the contact zone between the satellite droplet and the nuclear membrane, the deformation of the lamina, and what appears to be the dissolution of the lipid droplet’s phospholipid membrane as it merges with the main central lipid mass.
This is genuinely new in the context of lipedema. The researchers state explicitly that this is the first demonstration of this phenomenon in lipedema adipose tissue.
The lipomatosis argument
The deeper interpretive claim the paper makes is that the elevated frequency of Lochkerne — a feature associated with lipogenic tumors — supports classifying lipedema as a form of lipomatosis from a morphological perspective.
The word lipomatosis can sound either alarming or technical depending on your background, so let me be precise. Lipomatosis broadly refers to conditions characterized by abnormal, non-encapsulated overgrowth of adipose tissue — not simply obesity, but tissue-level structural abnormality in how fat accumulates and organizes. Madelung’s disease, familial multiple lipomatosis, and diffuse infiltrating lipomatosis are examples. Some researchers have already proposed placing lipedema within this spectrum, based on clinical and epidemiological reasoning, but concrete histological evidence has been limited. This paper is arguing that the cellular-level morphology now provides a more direct basis for that classification.
Critically, the researchers are not suggesting that lipedema is malignant. They found no lipoblasts — the cells that distinguish benign lipoma-like tissue from liposarcoma — in either lipedema or control samples. The nuclear atypia observed here refers to unusual shape and indentation, not features of malignant transformation. This distinction matters enormously, and the authors are careful to make it.
What matters is that lipedema adipocytes carry a structural signature that is, in the language of histology, more similar to lipogenic lesions than to normal fat tissue. That is a meaningful difference.
A convergence with genetics
One of the things I find most intellectually compelling about this paper is that it does not sit in isolation. It connects — indirectly, but suggestively — with a 2022 genome-wide association study by Grigoriadis and colleagues, which identified genomic variants near the LHFPL6 gene as being suggestively associated with lipedema, particularly familial forms. LHFPL6 is a member of the lipoma HMGIC fusion partner gene family — a gene family implicated in translocation-associated lipoma formation. The Salzburg researchers mention this explicitly: the cellular morphology they are observing, and the genomic signals pointing toward lipoma-related biology, are converging on the same territory.
This is not proof of mechanism. Two suggestive findings pointing in the same direction are not confirmation of a causal pathway. But as a researcher who has spent time working with genomic data, there is something worth sitting with here. When morphological evidence and genetic association evidence both point independently toward lipoma biology in lipedema, that is not easily dismissed. It invites serious follow-up.
What this does not tell us — and why that matters
I want to be honest about the limitations of this study, because I think intellectual honesty is what makes science trustworthy. The sample size is the most important constraint: nine lipedema patients and five controls is small. The statistical result is striking, but effect size estimates from small samples can shift considerably in larger cohorts. The finding needs replication, ideally in much larger groups with better-matched controls and richer clinical data.
The patient information available is also limited. We know the mean BMI (26.1 for lipedema, 22.8 for controls), mean age (33.8 and 44.4 years respectively), that none showed pronounced fibrosis, and that all were undergoing their first or second liposuction. But lipedema stage, disease duration, hormonal status, symptom severity, pain levels, nodule characteristics, family history, and genetic background are not reported. Lipedema is a heterogeneous disease, and a study of nine patients cannot tell us whether Lochkern frequency differs between early and late-stage disease, between women with and without family history, between different hormonal contexts, or between tissue from different body regions.
The tissue was also sampled from one specific anatomical location — the deeper subcutaneous layer of the extremities — and we cannot extrapolate from this to other layers or regions without further investigation.
Most fundamentally: this is a morphological study. It shows structure. It does not demonstrate function. The connections to lipogenesis, chromatin biology, gene expression, and lipoma genetics are intellectually motivated and scientifically plausible — but they are not yet demonstrated in lipedema tissue. The authors are proposing directions for future work, not reporting mechanistic conclusions.
The question of what nuclear deformation might actually do
The part of this paper that has stayed with me most is a short section in the discussion where the authors raise the possibility that the physical deformation of the adipocyte nucleus might have consequences for gene expression.
This is speculative — the paper does not contain transcriptomic data, epigenetic profiling, or any functional molecular measurements. But the reasoning is grounded in real cell biology. We know that the nucleus is not simply a passive container for DNA. Its three-dimensional shape, its mechanical environment, and the organization of chromatin inside it are all connected to how genes are regulated. A 2023 paper by Ivanovska and colleagues (cited by the Salzburg group) showed in adipogenically induced cells that small lipid droplets are physically rigid enough to indent the nucleus, dilate the nuclear lamina, and in some cases cause nuclear rupture — with associated DNA damage and disruption of repair mechanisms. The Salzburg team did not observe nuclear rupture in lipedema samples, but they raise the reasonable question of whether the degree of deformation they did observe might be sufficient to reorganize chromatin and alter transcriptional patterns.
Again: this is a hypothesis, not a finding. But it points toward a genuinely fascinating direction. If future studies can combine ultrastructural microscopy with single-cell transcriptomics in lipedema tissue, it may become possible to ask whether adipocytes carrying Lochkerne express different genes than those that do not — and whether those differences intersect with what we already know about inflammation, lipid metabolism, adipogenesis, extracellular matrix biology, or estrogen signaling in lipedema tissue.
What this means for those of us living with lipedema
I want to end with something that is neither hype nor dismissal, because I think both would be wrong here.
This study does not give us a new treatment. It does not tell us what causes lipedema. It does not tell us how to manage our symptoms differently. In clinical practice right now, Lochkerne are not a diagnostic criterion and could not be assessed in routine care.
What it does is contribute something genuinely important to the longer project of establishing that lipedema is a biologically serious disease with measurable structural differences at the cellular level. Differences that are independent of BMI. Differences that show up inside the fat cells themselves — inside the nucleus of the fat cell — and that resemble features previously associated with lipoma biology rather than ordinary adipose tissue.
For those of us who have spent years being told that our tissue is “just fat,” that sentence is not nothing. Diseases become harder to dismiss when their abnormalities can be seen under a microscope, quantified, and published. We are moving, incrementally but genuinely, toward a biology of lipedema that matches the lived experience of the disease.
The researchers — Steiner, Rinnerthaler, Mueller, Russe, Lipp and Bauer — deserve credit for approaching lipedema tissue with the technical seriousness it warrants, for being transparent about limitations, and for not overclaiming what their data show. That is the kind of research the lipedema community needs: careful, methodologically rigorous, and deeply curious about what is actually there when you look closely enough.
What they found, when they looked closely enough, was something strange and unexpected and worth following.
Thank you for being here and for supporting this work. LipedemaScience exists because I believe that every woman living with lipedema deserves access to the real science — not simplified away, not hidden behind paywalls she cannot afford, not filtered through voices that do not understand what it feels like to live in this body. Making complex research readable, honest and human is my passion, and it is something I pour myself into with every single piece I write. Your support is what makes it possible for me to keep doing this — not just for you, but for the woman who was just diagnosed last week, for the teenager who does not yet have words for what is happening to her, and for everyone who has ever been told that this is just fat. It is not just fat. And together, we are going to keep proving that.
Adipocytes from lipedema adipose tissue show lipoma-associated nuclear atypia (DOI: 10.3389/fcell.2026.1804040)
thank you, articles like this are exactly what I signed up for 💜
Thank you so very much for this, Carina! I have just enough science education to almost understand a lot of it—and I like that it pushes me further. I was diagnosed four weeks ago today so I’ve been on the Bullet Train to somewhere trying to learn and adopt all I can. Fortunately, for the past 15months, I’ve been following and learning from Dr William Li and adopted the Lumen metabolic process, so I’ve actually been doing the right things instead of just living, at age 77, with the ‘why don’t you just eat less and exercise more?’ Well, I did that, too, lost over 100 pounds over the past few years…and here I am putting more of the puzzle pieces on the table and in play. I very much admire and appreciate your work and your careful appraisals. Thank you!