
Redox, Oxidative Stress and Lipedema
A piece of biochemistry I first learned during my bachelor’s degree in nutrition may help us understand how energy production, blood vessels, inflammation and pain could intersect in lipedema.

Redox was one of the mechanisms I learned about while studying for my bachelor’s degree in nutrition. At the time, it belonged to the more demanding part of biochemistry: electrons moving between molecules, NADH, mitochondria, antioxidant enzymes and reaction pathways that seemed very far removed from everyday life.
But redox reactions are not a minor detail hidden inside a textbook. They are happening in us every second. They allow our cells to turn food into energy, help immune cells respond to infections and influence how blood vessels, nerves and tissues communicate.
Years later, as I started reading more about lipedema, I found myself returning to redox biology. Not because oxidative stress has been proven to cause lipedema. It has not. But because redox reactions sit at the centre of several processes that may be relevant to our symptoms: mitochondrial activity, vascular permeability, inflammation, bruising, pain and tissue remodelling.
What is a redox reaction?
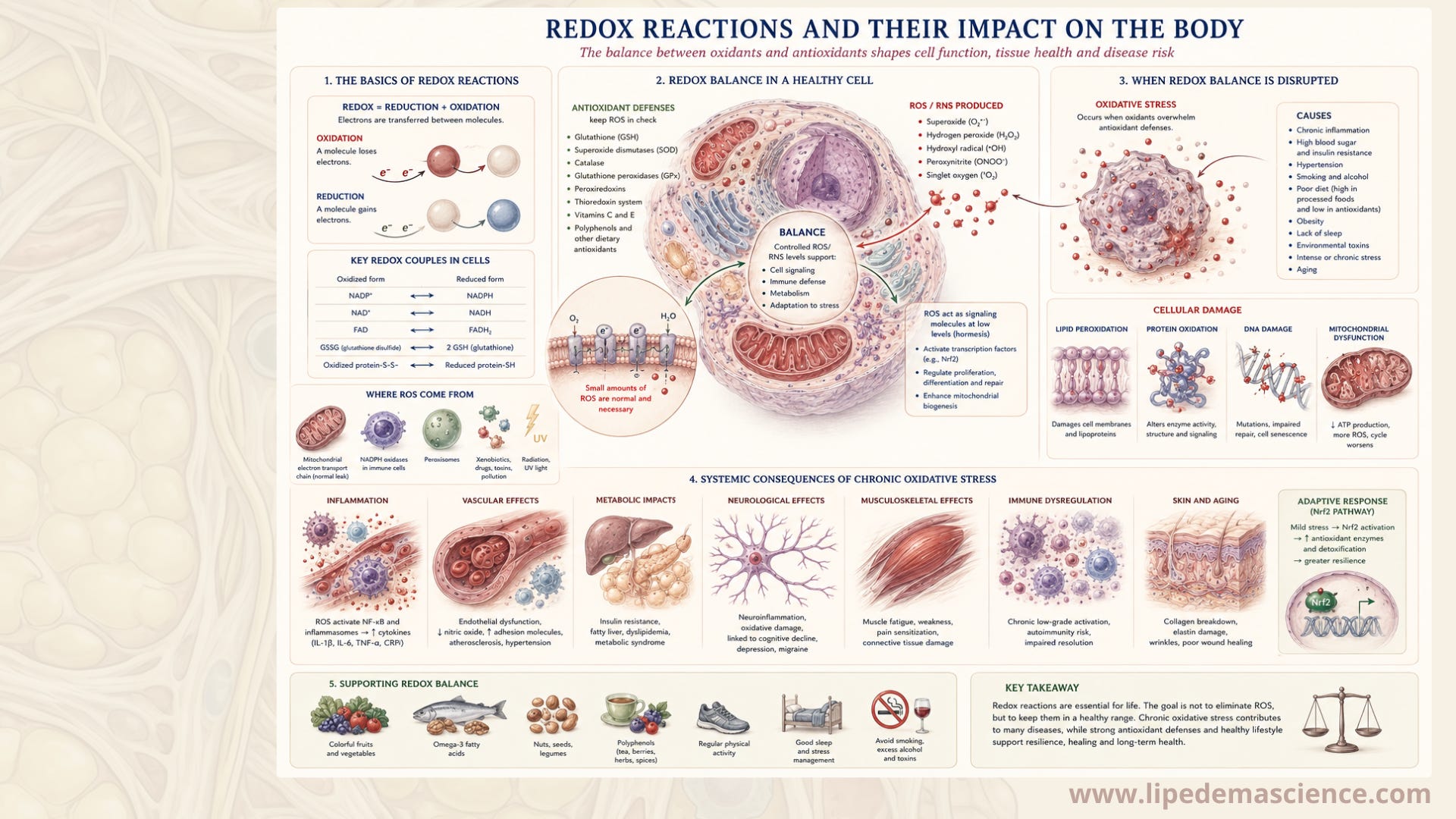
The word redox comes from reduction and oxidation. It describes a reaction in which electrons move from one molecule to another. The molecule losing electrons is oxidised. The molecule receiving them is reduced. The two processes always happen together.
This movement of electrons is what makes energy production possible. When we metabolise carbohydrates, fats and proteins, electrons are transferred to carriers such as NADH and FADH₂. These molecules transport them into the mitochondria, where they pass through the electron transport chain.
Oxygen receives the electrons at the end of the chain, and the energy released during the process is used to produce ATP, the form of energy our cells can use. In other words, our metabolism depends on controlled oxidation.
When oxygen becomes reactive
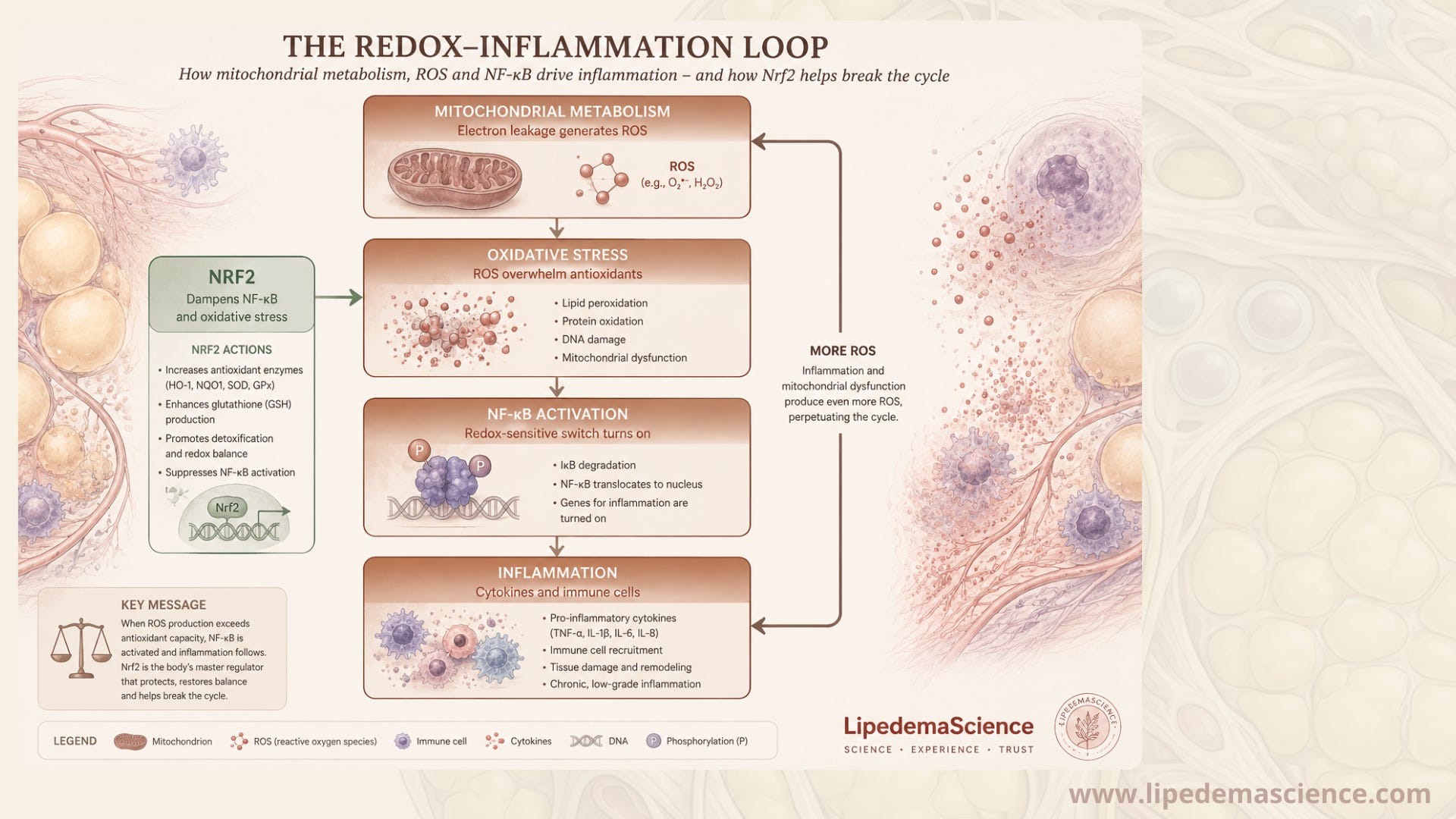
The transfer of electrons inside the mitochondria is not perfectly contained. Some electrons can escape and react with oxygen before reaching the end of the chain. This creates reactive oxygen species, commonly called ROS.
You may have heard ROS described as harmful waste products, but that is only part of the story. At normal levels, they act as signals. They help regulate immunity, blood-vessel function, tissue repair and the adaptations we gain from exercise.
The problem begins when ROS production becomes greater than the body’s ability to control it. This is what we call oxidative stress. When that happens, reactive molecules can begin to modify fats, proteins and DNA. The fats in cell membranes are particularly vulnerable, as oxidation can start a chain reaction known as lipid peroxidation.
The body has several systems designed to prevent this. Glutathione, superoxide dismutase, catalase, glutathione peroxidase and peroxiredoxins all help control reactive compounds. Vitamins C and E also participate, but they are only smaller parts of a much larger internal defence network. The aim is not to remove all ROS. It is to keep the system in balance.
What affects redox balance?
Redox balance changes according to what the body is dealing with. Our mitochondria produce more energy when demand rises, such as during physical activity. Immune cells deliberately produce ROS when they need to destroy microorganisms. Sleep loss, smoking, air pollution, persistent high blood sugar, illness and some forms of chronic stress can also increase oxidative pressure.
Nutrition matters, but not because one “superfood” can neutralise oxidative stress. The body needs protein and micronutrients to build its own defence systems. Glutathione contains amino acids, while several antioxidant enzymes depend on nutrients such as selenium, zinc, copper and manganese.
This does not mean that taking large doses of these nutrients will automatically improve the system. Too little can be a problem, but too much can also disturb normal biology.
Physical activity is a good example of why the conversation is more complicated than “oxidation is bad”. Exercise produces a temporary increase in ROS. These molecules then help signal the body to strengthen its mitochondria and increase its own antioxidant capacity. A small, controlled challenge can make the system more resilient.
Why might this matter in lipedema?
Much of what we know about oxidative stress in fat tissue comes from obesity research. In metabolically unhealthy obesity, enlarged fat cells, impaired blood flow, inflammation and mitochondrial stress may reinforce one another. It is tempting to place lipedema inside the same model. But lipedema is not simply obesity located in the legs.
Lipedema has its own pattern. The tissue is often painful and tender. Bruising can happen easily. Fluid handling and the small blood vessels appear to be affected. At the same time, many women with lipedema have relatively good glucose regulation and other signs of preserved metabolic health.
A few small studies have found higher levels of markers connected with lipid oxidation in the blood of women with lipedema. They have also found increased activity of antioxidant enzymes such as superoxide dismutase and catalase.
That could mean the body is experiencing greater oxidative pressure. It could also mean the defence system is responding appropriately. Blood tests cannot tell us exactly where the signal came from, and they do not prove that oxidative stress causes lipedema.
More recent tissue studies have complicated the story further. Some have found increased expression of pathways involved in mitochondrial respiration and energy production, together with less classical immune activation than researchers might expect.
So the honest answer is that we do not yet know whether mitochondria in lipedema are struggling, compensating or behaving differently for another reason.
The blood vessels may be especially important
One area I find particularly interesting is the relationship between fat tissue and the smallest blood vessels. Research suggests that signals from lipedema tissue can make endothelial cells, which form the inner lining of blood vessels, more permeable. A weaker vascular barrier could allow more fluid and proteins to move into the surrounding tissue.
Redox reactions are known to influence endothelial cell junctions, nitric oxide signalling and blood-vessel function in other conditions. It is therefore plausible that local redox signals could be involved in the vascular changes seen in lipedema.
But plausible is not the same as proven. Researchers have found altered permeability. They have not yet shown that ROS are the cause. Still, this could be one place where the pieces meet: altered tissue signals, more vascular leakage, increased tissue pressure and greater stress on nerves and connective tissue.
Could bruising create local oxidative stress?
The tendency to bruise easily also raises an interesting question. When red blood cells escape from a damaged vessel, haemoglobin and iron must be cleared from the tissue. Iron is essential, but when it is poorly controlled it can take part in reactions that produce highly reactive radicals.
Macrophages help clean up haemoglobin and damaged cells. Lipedema tissue appears to contain many CD163-positive macrophages, a type involved in tissue repair and the handling of blood products.
Could repeated microscopic bleeding create local episodes of iron-related oxidative stress? Could that contribute to tenderness or tissue remodelling?
At the moment, this is a research hypothesis rather than an established explanation. But it connects a very recognisable symptom - easy bruising - with a biological process that could be measured in future studies.
Redox and pain
Redox biology may also be relevant to pain. Products formed when fats are oxidised can influence sensory nerves. In other pain conditions, reactive molecules can make nerve endings more sensitive and lower the threshold at which they begin to signal pain.
In lipedema, this could interact with swelling, pressure, fibrotic tissue and mechanical stress. Redox products may not create the problem alone, but they could amplify pain in tissue that is already vulnerable. Again, this has not been demonstrated directly in lipedema. We need studies that measure oxidised lipids and redox-sensitive pain pathways inside affected tissue.
Where hormones may fit
Lipedema frequently appears or changes around puberty, pregnancy and menopause, which makes hormonal biology difficult to ignore.
Oestrogen can influence fat-cell development, blood vessels, mitochondrial activity and the body’s antioxidant systems. Early lipedema studies have found changes in genes involved in local oestrogen metabolism.
This creates a possible connection between hormonal transitions and redox regulation. A change in local oestrogen signalling could alter how cells use energy, respond to stress or maintain the vascular barrier.
But the full chain has not been established. We cannot yet say that oestrogen causes oxidative stress in lipedema, or that redox imbalance explains the hormonal pattern of the disease.
What can we do with this information?
The practical message is not that everyone with lipedema should start taking antioxidant supplements. There is currently no evidence that high-dose antioxidants treat lipedema. More is not necessarily better, and very large doses may interfere with useful redox signals, including some of the signals involved in exercise adaptation.
A better approach is to support the systems the body already uses:
Eat enough protein and a varied diet containing vegetables, fruit, nuts, seeds, fish, eggs and other nutrient-dense foods that suit you.
Stay physically active in ways your body tolerates. Walking, strength training, swimming and other regular movement can support mitochondrial and vascular health.
Prioritise sleep and recovery, especially during periods when symptoms are worse.
Avoid smoking and limit unnecessary exposure to pollutants where possible.
Manage blood sugar and body weight without assuming that lipedema can be dieted away.
Correct confirmed nutrient deficiencies with appropriate guidance rather than taking large doses “just in case”.
None of these removes lipedema. But they may improve the general environment in which our cells, blood vessels and tissues have to function. For me, that is a more useful way to think about redox health than searching for the strongest antioxidant supplement.
Redox reactions are not the enemy. They are the chemistry that keeps us alive. There are early signs that oxidative balance may be altered in lipedema, but the evidence is still limited and sometimes contradictory. The most likely explanation may not be a dramatic, whole-body state of oxidative stress.
Instead, redox biology may matter locally around small blood vessels, macrophages clearing damaged cells, sensitive nerve endings and mitochondria adapting to changes in the tissue.
It may not be the mechanism that starts lipedema. But it could influence how the tissue responds, how much it leaks, how easily it bruises and how painful it becomes. That is still only part of the picture. But it is a part worth studying.
