
More Than “Calories In, Calories Out”
Why metabolism, hormones, and fat biology make weight regulation different for women with lipedema. A new way to understand energy and weight.

For many years, we were told that body weight simply comes down to “calories in versus calories out.” Eat less, move more, and the body will respond. But modern science shows that this view is far too simple—especially for women living with lipedema.
The human body is not a calculator. It’s a living system that constantly adjusts how it burns, stores, and uses energy depending on hormones, inflammation, genetics, and even the health of our gut. Understanding this complexity can help shift our focus from blame and frustration to awareness and self-acceptance.
Food isn’t “inside your body” until it crosses the gut wall
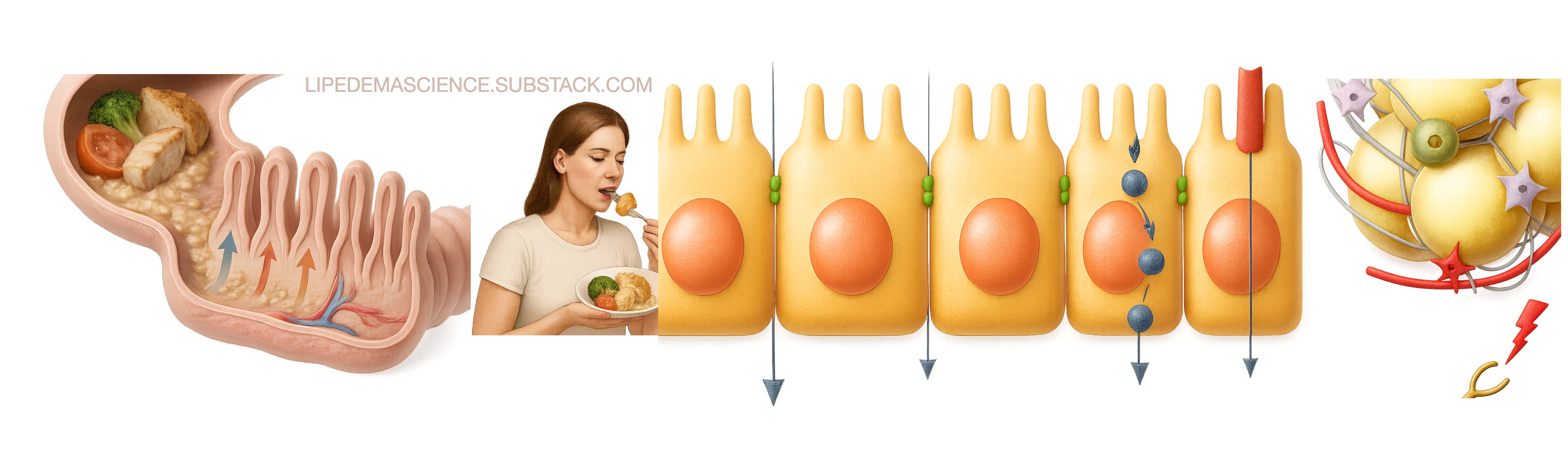
A basic but powerful fact: food that’s still inside your digestive tract isn’t technically “in your body.” Only when nutrients pass through the intestinal wall and enter the bloodstream can they be used for energy or stored as fat.
This means that digestion, absorption, gut bacteria, and inflammation can all change how much energy your body actually gets from what you eat. Two people can eat the same meal, but their bodies might absorb and process it very differently.
Hormones shape how energy is used
Hormones act like the body’s traffic lights for energy flow. Insulin directs nutrients into storage, cortisol mobilizes them during stress, and thyroid hormones set the pace of metabolism. For women, estrogen and progesterone add another layer, influencing where fat is stored and how sensitive cells are to insulin.
In lipedema, research has shown that fat cells in the affected areas respond abnormally to these hormonal signals. Genes such as AKR1C1, involved in progesterone metabolism, and processes linked to inflammation and extracellular matrix changes, can make this tissue resistant to fat loss—even when calories are reduced.
Lipedema fat behaves differently
Several studies show that lipedema tissue is biologically distinct from regular fat. It has chronic low-grade inflammation, higher estrogen sensitivity, and altered insulin signaling. The hypertrophic fat cells in the legs and arms can grow and store energy even when the rest of the body loses weight.
This explains why many women say: “I lose weight everywhere except my legs.” It’s not a failure of willpower—it’s how the tissue behaves on a cellular level.
When “less food” doesn’t mean “less fat”
Reducing calories does not always translate into fat loss in lipedema areas. The body adapts by lowering energy expenditure, increasing hunger hormones, and preserving the very fat it perceives as essential. Over time, this can lead to frustration, fatigue, and even weight regain, not because of a lack of effort but because of built-in metabolic defense systems.
Scientists now emphasize the quality of food—its effect on hormones and inflammation—over strict calorie counting. Diets that lower the glycemic load (fewer processed, fast-absorbed carbohydrates) and support hormonal balance tend to reduce cravings and stabilize metabolism better than simply “eating less.”
Acceptance through understanding
Learning that weight regulation is not just about numbers can bring a sense of relief. Lipedema is not a reflection of discipline or morality—it’s a condition with clear biological roots. Understanding that hormones, genetics, and tissue biology play major roles helps replace guilt with compassion.
Acceptance does not mean giving up; it means working with your body instead of against it. Supporting lymph flow, managing inflammation, nourishing with balanced meals, and caring for mental well-being can all help the body function more harmoniously.
A more compassionate view
“Calories in, calories out” gave us a rule. Science gives us a story—a deeper understanding of why our bodies act the way they do. For women with lipedema, that story is one of resilience, complexity, and biology, not failure.
When you understand your body’s language, you can finally stop fighting it—and start taking care of it in the way it deserves.
Transcriptomics of Subcutaneous Tissue of Lipedema Identified Differentially Expressed Genes Involved in Adipogenesis, Inflammation, and Pain (DOI: 10.1097/GOX.0000000000006288)
Lipedema: Insights into Morphology, Pathophysiology, and Challenges (DOI: 10.3390/biomedicines10123081)
The carbohydrate-insulin model: a physiological perspective on the obesity pandemic (DOI: 10.1093/ajcn/nqab270)
Aldo-Keto Reductase 1C1 (AKR1C1) as the First Mutated Gene in a Family with Nonsyndromic Primary Lipedema (DOI: 10.3390/ijms21176264)
Therapeutic use of intermittent fasting for people with type 2 diabetes as an alternative to insulin (DOI: 10.1136/bcr-2017-221854)
Hyperinsulinemia and Insulin Resistance: Scope of the Problem (DOI: 10.4102/jir.v1i1.18)
Therapeutic use of intermittent fasting and ketogenic diet as an alternative treatment for type 2 diabetes in a normal weight woman: a 14-month case study (DOI: 10.1136/bcr-2019-234223)
The Carbohydrate-Insulin Model of Obesity: Beyond “Calories In, Calories Out” (DOI: 10.1001/jamainternmed.2018.2933)
Dr. David Ludwig clears up carbohydrate confusion (https://nutritionsource.hsph.harvard.edu/2015/12/16/dr-david-ludwig-clears-up-carbohydrate-confusion/)
Weight-loss maintenance--mind over matter? (DOI: 10.1056/NEJMe1011361)
The glycemic index: Reports of its demise have been exaggerated (DOI: 10.1002/oby.21125)