
Menopause and Lipedema: The Fire Beneath the Blood Test
Why normal blood tests may miss the local estrogen activity, receptor imbalance, inflammation and fibrosis happening inside lipedema fat.

Over the past couple of years, so many people have asked me about lipedema and menopause. I am not there yet myself, but the question has come up almost weekly from women all over the world, and I finally felt that I needed to dig deep.
There is a particular kind of frustration that many women with lipedema know from perimenopause. Something changes. The pain sharpens. The heaviness deepens. The tissue feels different, less forgiving, harder to move through. So you go to your doctor, your levels are checked, and you are told: everything looks fine.
Normal. Within range. Nothing to worry about.
And you leave the appointment carrying both the test result and your body’s testimony, trying to reconcile two things that seem to be describing completely different realities.
That contradiction is not in your head. It is not anxiety about getting older, or a failure to accept change, or something that will resolve with the right mindset. It has a biological explanation — one that standard hormone panels were simply never designed to find. And understanding it, really understanding it, changes the entire way you see what is happening inside you.
The conversation your blood test cannot have
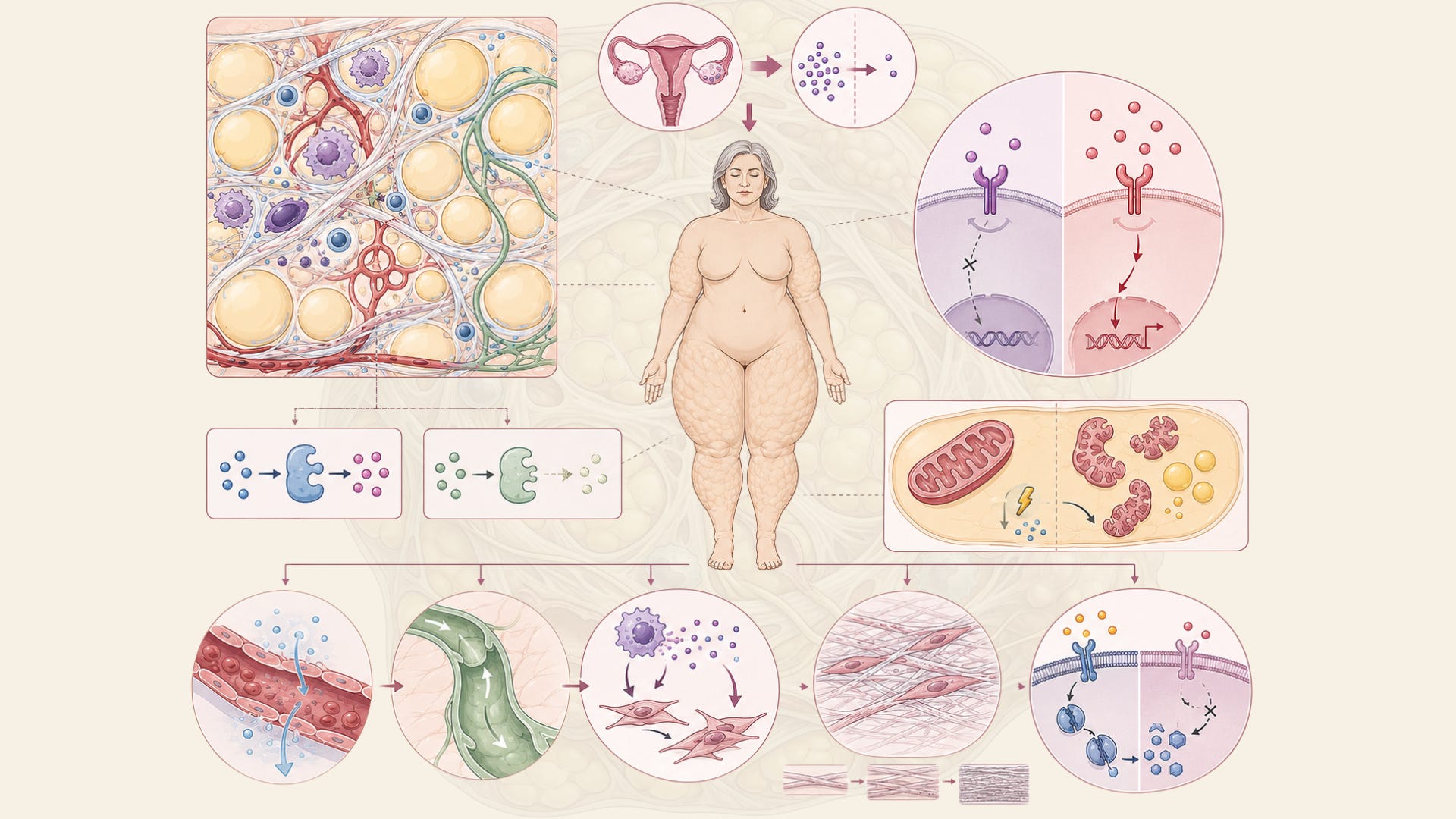
When a doctor measures your hormone levels, they are measuring what is circulating in your bloodstream at a given moment. That information is real and it matters. But it tells you almost nothing about what is happening inside lipedema adipose tissue specifically — because lipedema fat is not passive. It is a biologically active environment with its own local hormonal economy, its own enzyme systems, and increasingly, its own estrogen production. The blood and the tissue are having two completely separate conversations.
Since so many people are asking similar questions about lipedema and menopause, I would really recommend leaving your question in the comments. That way, every subscriber can see the answer, and we can build a shared discussion that helps more people understand this topic better.
This is the central insight from a 2025 narrative review published in the International Journal of Molecular Sciences. The paper — titled “Menopause as a Critical Turning Point in Lipedema: The Estrogen Receptor Imbalance, Intracrine Estrogen, and Adipose Tissue Dysfunction Model” — is one of the most detailed attempts yet to map the molecular landscape of why menopause so often acts as an accelerant in lipedema. It is a hypothesis-driven review, not a clinical trial, and I want to be precise about that. But it draws on converging lines of evidence from earlier studies and constructs a model that is difficult to dismiss — and that, in my view, every woman with lipedema navigating perimenopause deserves to know about.
Two receptors, one imbalance
To understand the model, you need to know a little about how estrogen actually works inside fat tissue. Estrogen does not simply arrive and act uniformly. It binds to specific receptor proteins inside cells, and different receptors drive very different outcomes. The two main ones in adipose tissue are called estrogen receptor alpha (ERα) and estrogen receptor beta (ERβ), and they are not interchangeable.
In healthy adipose tissue, ERα is broadly considered the metabolically protective receptor. When it is active and functioning well, it supports healthy fat metabolism, helps regulate lipid oxidation, supports mitochondrial function, and generally keeps the tissue behaving in an orderly, responsive way. ERβ, by contrast, appears to promote a different type of cellular environment — one more associated with fat accumulation, increased inflammation, reduced lipolysis, and tissue fibrosis when it becomes dominant.
For some years now, researchers studying lipedema have noticed that this receptor balance is already disrupted in lipedema tissue. Earlier work, including an influential 2021 review in the International Journal of Molecular Sciences, proposed that dysregulation of estrogen receptor distribution — specifically a shift in the ERα/ERβ ratio — might drive the altered fat metabolism seen in lipedema. According to that model, reduced ERα activity could increase the activation of PPARγ (a transcription factor that promotes fat cell differentiation and fat storage), drive free fatty acids into adipocytes, suppress lipolysis, impair mitochondrial biogenesis, and stimulate angiogenesis — collectively creating the biological conditions for disproportionate fat accumulation.

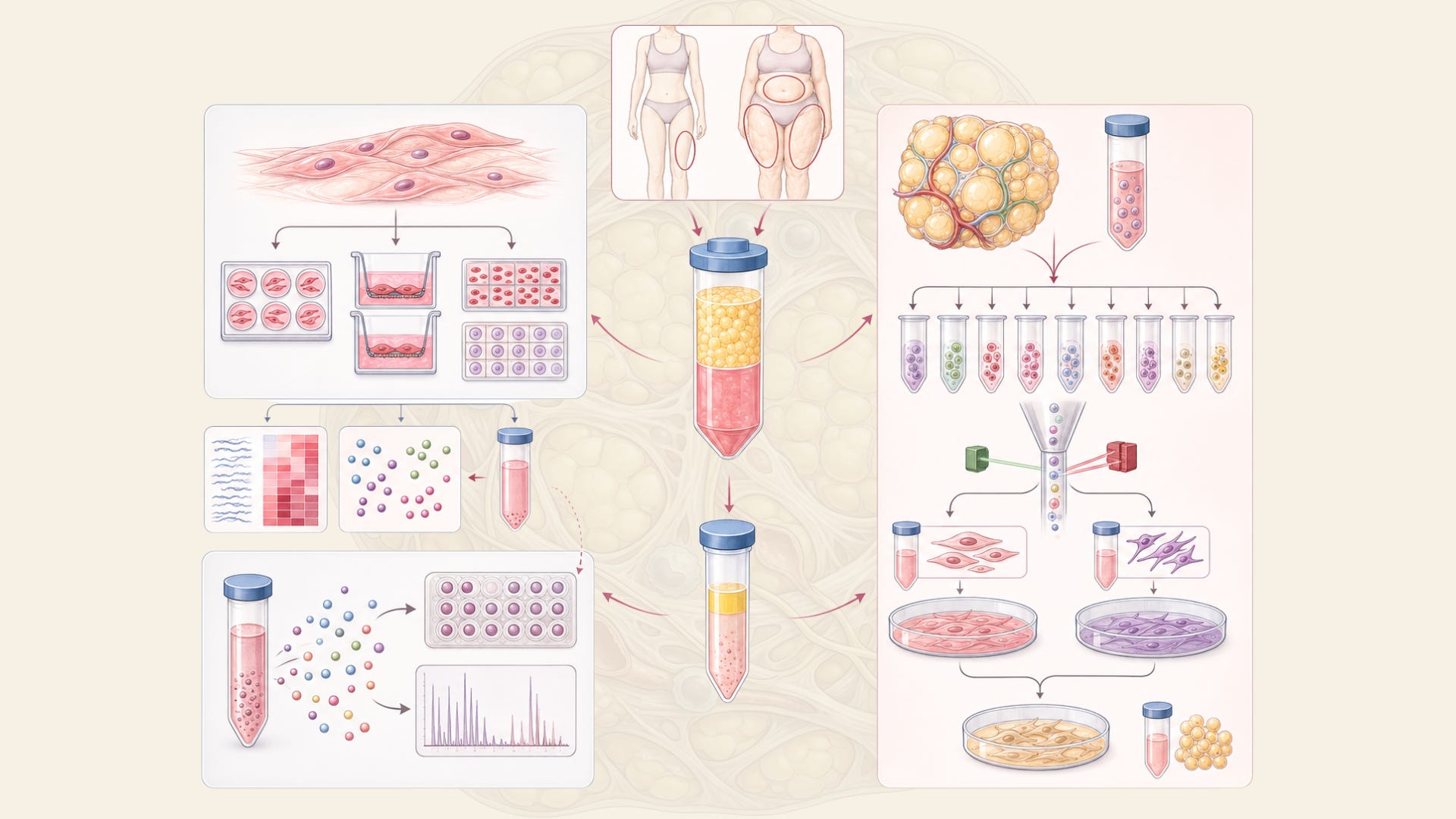
That hypothesis gained further molecular grounding from a 2024 cell study published in Obesity, who examined estrogen receptor gene expression in adipose-derived stem cells (ASCs) and three-dimensional spheroid cultures from women with lipedema compared to BMI- and age-matched healthy controls. Their findings were striking: ERβ gene expression was significantly elevated in hormone-depleted lipedema ASCs and spheroids compared to healthy cells. ERα and GPER — a third estrogen receptor — were significantly decreased in estrogen-treated lipedema spheroids. Lipedema cells, in other words, were already wired differently at the receptor level. The study also found altered expression of CYP19A1, the gene that encodes the enzyme aromatase — something I want to come back to, because it becomes central to the menopause story.
This was a cell study, so the findings reflect what happens in isolated adipose-derived cells in laboratory conditions rather than in living tissue in a complex human body. Cell studies are important starting points, not endpoints. But the pattern they revealed aligned closely with what other researchers had been proposing on theoretical grounds.
What menopause actually does to this already-disrupted system
Here is where the 2025 review adds the most important layer. If lipedema tissue already has an ERα/ERβ imbalance, what happens when menopause arrives and systemic estrogen begins to fall?
The intuitive answer might be: less estrogen, less problem. But the biology goes in a more complicated and, frankly, more difficult direction.
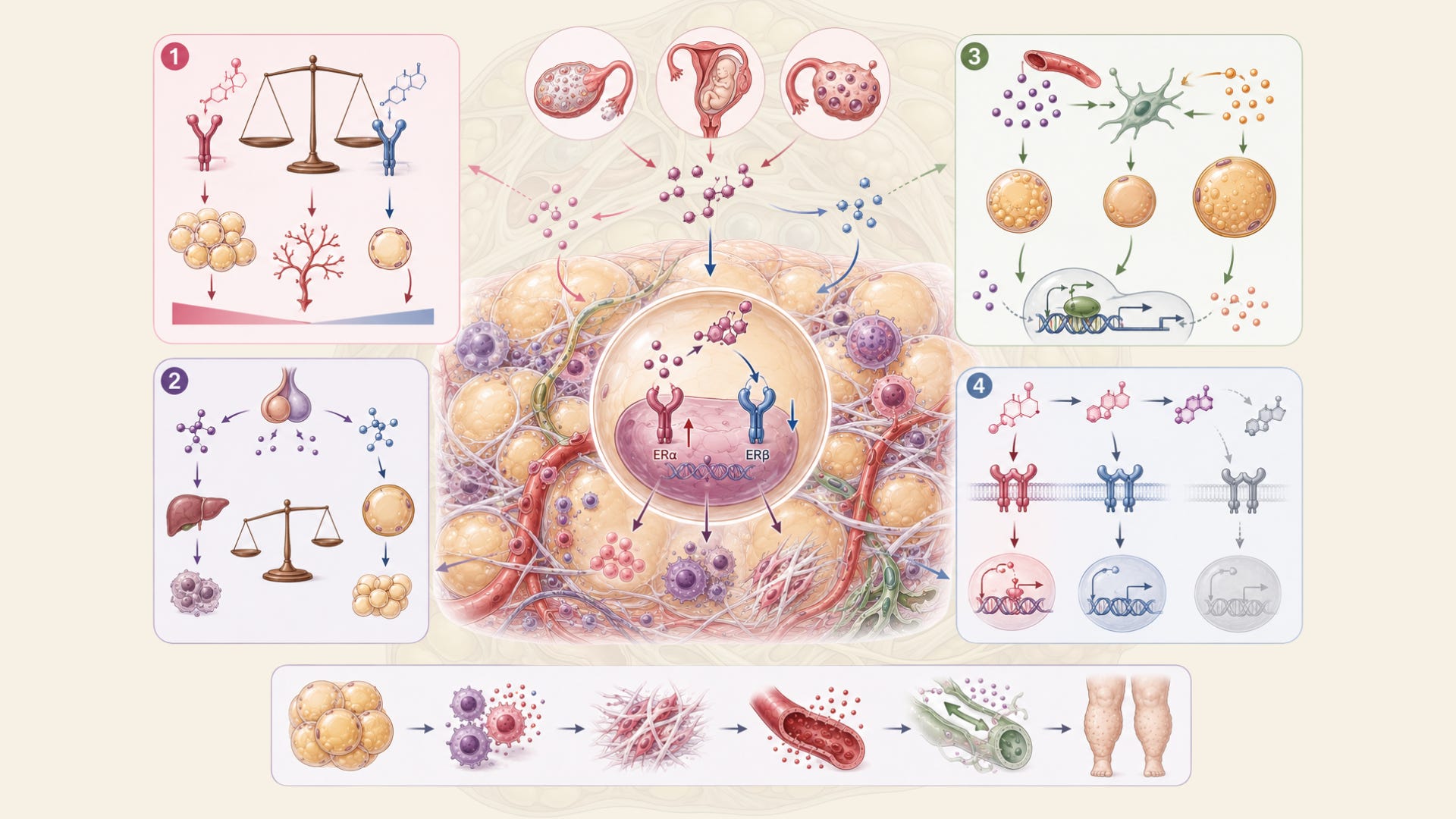
According to the proposed model, the decline in circulating estrogen that comes with menopause does not calm the tissue down. Instead, it amplifies the existing imbalance. ERα signaling — already relatively weak in lipedema — becomes further suppressed. ERβ activity is further enhanced. The protective receptor retreats and the receptor more closely associated with fat accumulation, inflammation, and fibrosis becomes more dominant. Mitochondrial function worsens. Insulin sensitivity in the tissue declines. The capacity to oxidize fat decreases. And all of this unfolds in tissue that was already struggling to maintain metabolic balance.

But there is a second mechanism at work here, and it is the one that I think is most important for understanding why the blood test and the body’s reality can be so completely at odds.
The tissue keeps making its own estrogen
Adipose tissue does not just respond to estrogen arriving from the circulation. It also produces estrogen locally, through a system of enzymes that can convert precursor hormones directly within the tissue cells. This is called intracrine signaling — and it is one of the most consequential concepts for understanding lipedema around menopause.
The key enzyme here is aromatase, encoded by the CYP19A1 gene. Aromatase converts androgens into estrogens locally, inside the fat tissue itself. The 2025 review proposes that in lipedema adipose tissue, aromatase activity is upregulated — meaning the tissue is producing more local estrogen even as circulating estrogen falls. This was supported by findings from an earlier early-stage lipedema tissue study published in Biomedicines in 2022, which found altered aromatase gene expression in lipedema stromal vascular fraction cells even at early disease stages, alongside evidence of endothelial barrier disruption — suggesting that the hormonal alterations are present early and are embedded in the tissue’s cellular architecture.
The 2025 review describes a further enzymatic imbalance: 17β-hydroxysteroid dehydrogenase type 1 (17β-HSD1), which converts weaker estrogens into the more potent estradiol, is reportedly upregulated in this model. Meanwhile, 17β-HSD2, the enzyme that performs the reverse conversion — inactivating estradiol back into a weaker form — is suppressed. The net result, according to this proposed mechanism, is a sustained excess of local estradiol inside the tissue, even after blood estrogen has fallen to postmenopausal levels.
The fire, in other words, does not go out when the systemic supply drops. It shifts inward, sustains itself through local enzyme activity, and continues driving the inflammatory, fibrotic, and metabolically disruptive processes that characterize advanced lipedema. Your blood test measures the flame it can see. It has no way to see what is burning underground.
A molecular signature that is beginning to look familiar
One of the most scientifically interesting aspects of the review is a comparison that has been quietly building in the lipedema literature for a few years. The authors note that the molecular signature observed in lipedema — local estrogen excess, ERα suppression, ERβ dominance, intracrine estrogen production through aromatase overactivity, and downstream inflammation and fibrosis — closely mirrors the biology seen in other estrogen-driven gynecological conditions, including endometriosis, adenomyosis, and uterine fibroids.
This is not a coincidence, and it is not something the authors mention casually. It is part of a broader argument they are making: that lipedema may need to be reframed not simply as an adipose tissue disorder or a lymphatic disorder, but as an estrogen-receptor-driven gynecological disorder — one that shares fundamental molecular mechanisms with conditions that have long been taken more seriously in clinical medicine, because they affect reproductive organs rather than fat tissue.
A 2025 review in Archives of Plastic Surgery, which specifically examined hormonal links between lipedema and gynecological disorders and explored the potential therapeutic roles of gestrinone and drospirenone, reinforces this framing. It describes a common pathway involving estrogen receptor imbalance that links lipedema’s biology to these other conditions — not identically, but through recognizable molecular themes. The authors discuss how certain hormonal treatments already used for estrogen-driven gynecological conditions might theoretically be relevant to lipedema, though they are careful to note this is preliminary and requires clinical evaluation.
For me, as someone who has lived with lipedema since diagnosis in 2012 and who spent years in laboratory settings studying inflammation at the cellular level, this reframing matters enormously. It is not just academically interesting. It changes the legitimacy framework around lipedema. It suggests the tissue is not poorly behaved fat. It is tissue caught in a hormonal signaling loop that, under the right molecular conditions, cannot easily regulate itself.
What this model still does not answer
Scientific honesty requires that I say this clearly: the 2025 paper is a narrative review — a synthesis of existing research into a proposed model. It is not a randomized trial. It is not a clinical outcome study. The mechanisms it describes — the receptor imbalance, the intracrine estrogen loop, the enzymatic shifts — are proposed based on converging evidence from cell studies, earlier mechanistic reviews, and molecular parallels with related conditions. They have not yet been confirmed through large-scale human tissue studies specifically designed to test these pathways in lipedema patients at different menopausal stages.
A 2026 systematic review on hormonal influences in lipedema, which screened 64 papers and ultimately included 15 for analysis, concluded that lipedema appears to be a multifactorial condition driven primarily by hormonal dysregulation — especially involving estrogen — alongside metabolic and possibly genetic components. It identified four main pathophysiological hypotheses in the literature, including changes in estrogen metabolism and receptor function, but also general hormonal imbalance, growth hormone changes, and metabolic imbalance involving adipokines and PPARγ. The review concluded that further research into diagnostic biomarkers and targeted therapies is urgently needed. Fifteen included papers is not a large evidence base, and the heterogeneity across studies remains significant.
So what we have is a biologically plausible, increasingly well-articulated model — supported by cell studies, gene expression data, mechanistic reviews, and molecular parallels with better-studied conditions — that has not yet completed the full translational journey from proposed mechanism to confirmed clinical protocol. That matters when you are trying to decide what to do with this information. It does not mean the model is wrong. It means it is not yet proven in the way that clinical medicine requires before it shapes treatment guidelines.
There is also important heterogeneity in lipedema itself that is easy to overlook in mechanistic reviews. Not all women with lipedema experience the same progression around menopause. Not all women with lipedema have the same disease stage, the same genetic background, the same metabolic profile, or the same hormonal history. A model constructed from averaged findings and proposed mechanisms may capture something real about the biology without capturing every woman’s individual experience. Research in this area remains in relatively early stages, and the lipedema field still lacks the large, prospective, well-controlled clinical studies needed to confirm or refine these mechanistic proposals.
What it means to understand this
I think there are two different ways this knowledge can land, and I want to name both of them.
The first is the purely intellectual one: this is a scientifically sophisticated explanation for why something real is happening, and it deserves to be taken seriously by clinicians and researchers. It gives lipedema a legitimate hormonal biology, not a mystery or a lifestyle failure or an inevitability to simply manage. If the proposed mechanisms hold under further study, they open genuine questions about whether hormonal modulation strategies developed for related conditions might eventually be evaluated in lipedema — and about what metabolic interventions might support the tissue environment in meaningful ways.
The second way this knowledge lands is more personal, and I think it matters equally. If you have been told your hormones are fine while your body tells you something very different, this research offers a biological framework for why both of those things can be simultaneously true. The blood test is not lying. But it is looking at the wrong place. The lipedema tissue has its own hormonal activity, its own enzymatic environment, its own internal dynamics — and a standard panel cannot see inside it.
That is not a small thing. It is the difference between being told there is no explanation and being told the explanation requires more sophisticated tools to find. One of those is dismissal dressed as reassurance. The other is the beginning of a real conversation.
Menopause may be a turning point for lipedema. But understanding the mechanism is itself a form of power — not because it offers a quick answer or a guaranteed treatment, but because it means you are no longer navigating in the dark.
You are seeing the terrain.
Since so many people are asking similar questions about lipedema and menopause, I would really recommend leaving your question in the comments. That way, every subscriber can see the answer, and we can build a shared discussion that helps more people understand this topic better.
Menopause as a Critical Turning Point in Lipedema: The Estrogen Receptor Imbalance, Intracrine Estrogen, and Adipose Tissue Dysfunction Model (DOI: 10.3390/ijms26157074)
Lipedema and the Potential Role of Estrogen in Excessive Adipose Tissue Accumulation (DOI: 10.3390/ijms222111720)
The Expression of Adipogenic Marker Is Significantly Increased in Estrogen-Treated Lipedema Adipocytes Differentiated from Adipose Stem Cells In Vitro (DOI: 10.3390/biomedicines12051042)
Multi-Level Analysis of Adipose Tissue Reveals the Relevance of Perivascular Subpopulations and an Increased Endothelial Permeability in Early-Stage Lipedema (DOI: 10.3390/biomedicines10051163)
Lipedema and adipose tissue: current understanding, controversies, and future directions (DOI: 10.3389/fcell.2025.1691161)
Impact of hormones on lipedema development: a systematic literature review (DOI: 10.1007/s00404-026-08318-1)
Hormonal Links between Lipedema and Gynecological Disorders: Therapeutic Roles of Gestrinone and Drospirenone (DOI: 10.9734/jammr/2025/v37i25731)