
Living with a Chronic Disease and an Eating Disorder
When a food sensitive chronic condition like lipedema shapes daily choices, eating can shift from nourishment to negotiation, control, and emotional strain.

When you live with a chronic disease that is influenced by food, your relationship with eating can become complicated. Not because you lack discipline. Not because you are weak. But because food becomes loaded with meaning.
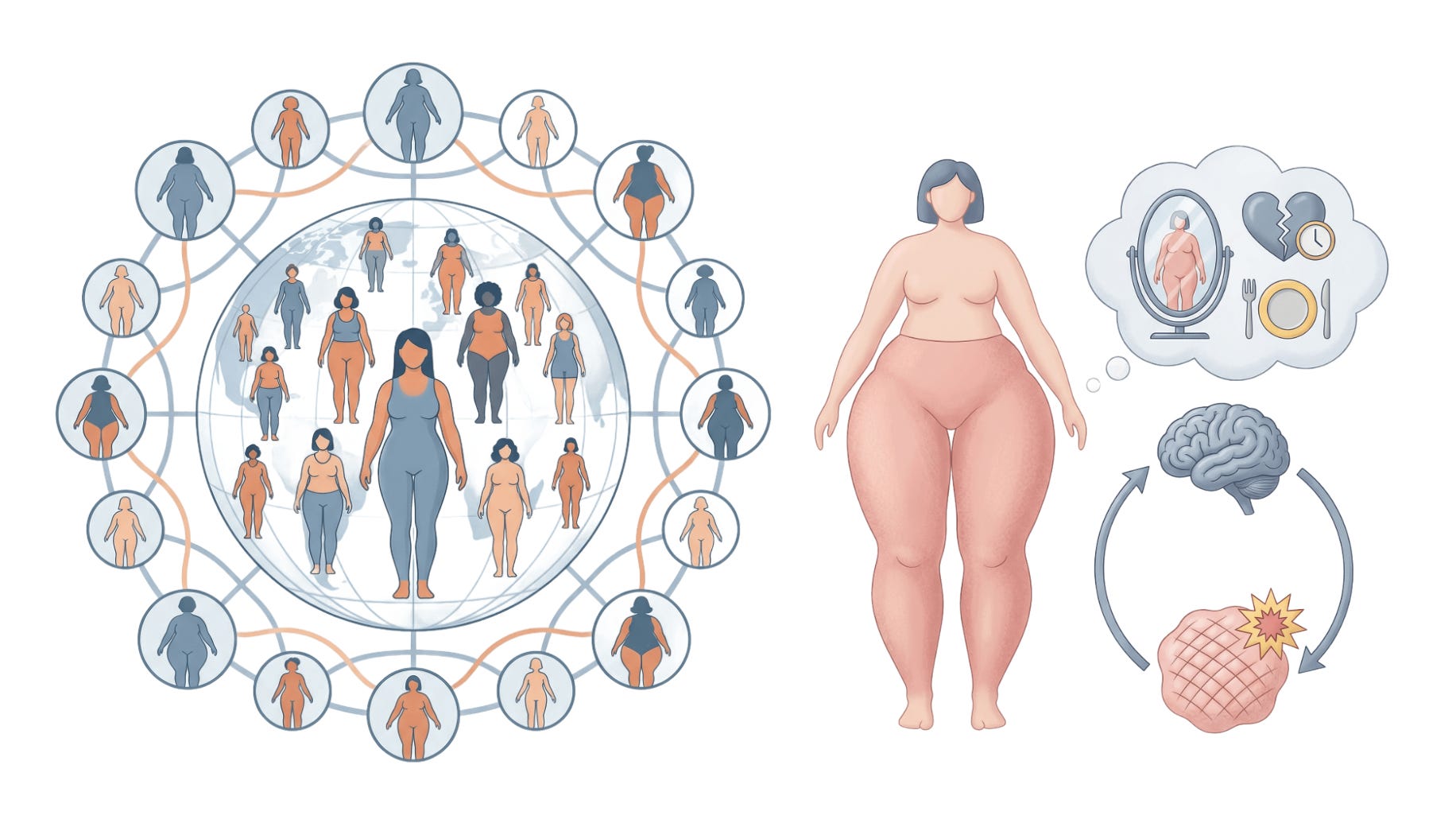
Lipedema affects a significant proportion of women worldwide. If we imagine roughly 4 billion women on this planet, and estimates suggest around 10-11 % may live with lipedema, we are not talking about a small niche group. We are talking about hundreds of millions of women across cultures, languages, socioeconomic backgrounds, and belief systems. Some diagnosed. Many not.
Behind every statistic is a woman trying to make sense of her body.
I am one of them…

A global condition, lived differently
There is no single “type” of lipedema woman.
Some have struggled with anorexia or restrictive eating. Others live with binge eating, emotional eating, or obesity. Some move between extremes over the course of years. Some have never had a complicated relationship with food at all.
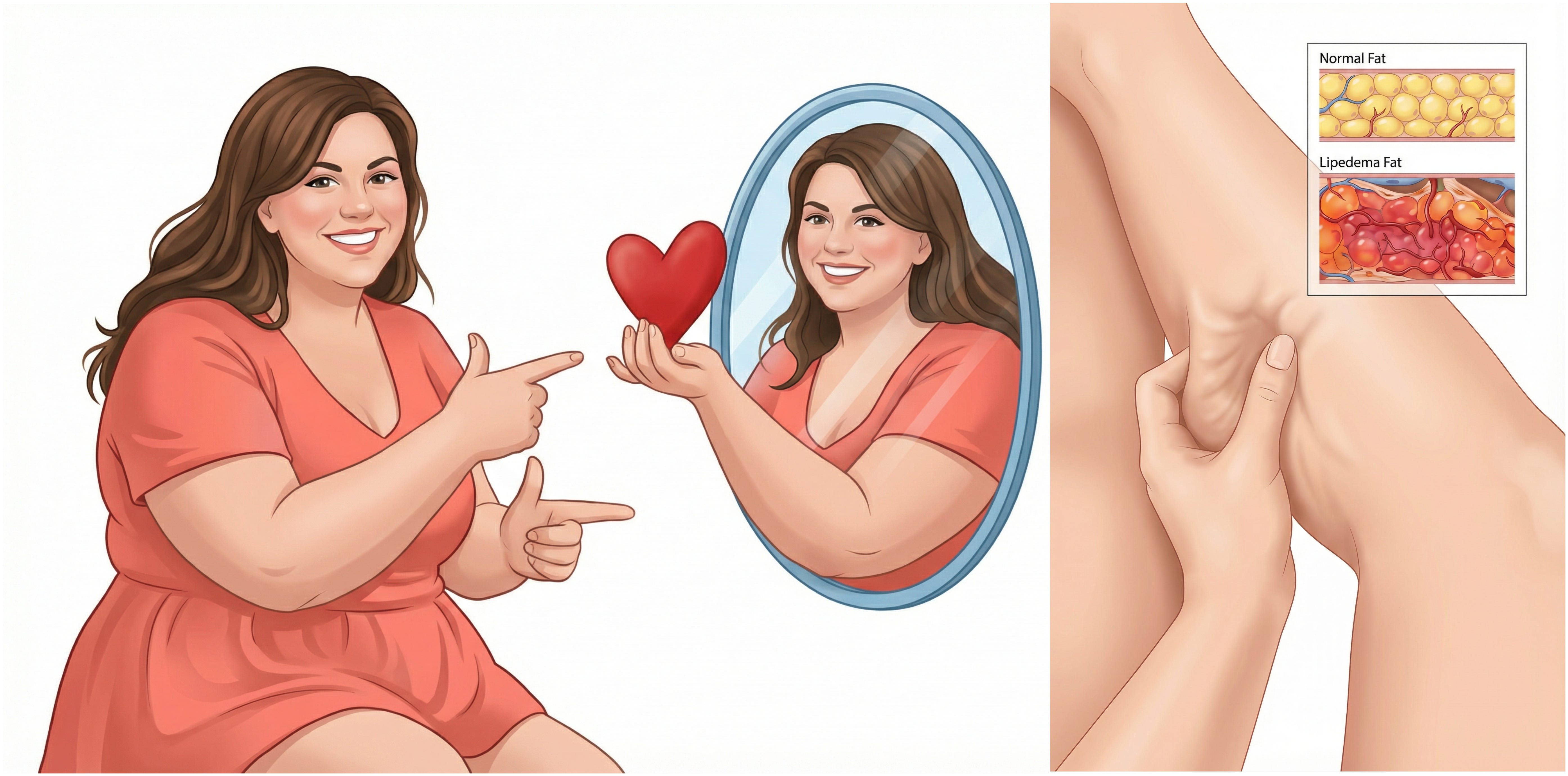
Lipedema is not obesity. That distinction matters. But lipedema can coexist with obesity, and when it does, the biological and psychological burden often increases. Lipedema tissue is associated with enlarged fat cells, inflammation, and progressive fibrosis. It is often resistant to traditional weight loss strategies.
When repeated efforts to lose weight do not change the characteristic fat distribution, frustration builds. Self blame creeps in. The narrative becomes personal.
For some, discovering that anti inflammatory or low carbohydrate approaches may reduce symptoms brings hope. For others, it becomes another arena for perfectionism, guilt, and social isolation. Strict dietary rules can feel empowering in the beginning. They can also become rigid, unforgiving, and mentally exhausting.
Living with lipedema in Brazil is not the same as living with it in Norway. Access to healthcare differs. Cultural body ideals differ. Food culture differs. Family expectations differ. But the psychological patterns can be strikingly similar. Shame. Isolation. The sense of fighting a body that does not respond the way you were told it should.
The psychological burden is real
Research increasingly shows that lipedema is associated with higher levels of depression, anxiety, emotional dysregulation, and reduced quality of life. Chronic pain, visible body changes, and frequent misdiagnosis amplify emotional strain.
Emotional regulation plays a central role. When feelings are overwhelming or unclear, food easily becomes a coping strategy. That can look like emotional eating. It can also look like strict restriction. Both can provide temporary relief. Both can reinforce long term distress.
Repeated unsuccessful dieting attempts are well known risk factors for disordered eating in the general population. In lipedema, where weight loss often does not substantially change lower body fat distribution, the psychological impact can be intensified.
Even at very low body weights, lipedema fat may persist. This biological resistance can escalate attempts at control. The body does not change as expected. The mind responds by pushing harder.
This is not a character flaw. It is a predictable human reaction to chronic stress and perceived loss of control.
Body image under pressure
Lipedema can profoundly affect body image. Disproportionate fat distribution, tenderness, and nodular tissue create a sense of a “diverging body.” Many women describe hiding their legs or arms. Others describe feeling trapped in a body that no longer feels like their own.
Misunderstanding from healthcare providers and society adds another layer. When lipedema is dismissed as simple obesity, women internalize blame. The gap between effort and outcome becomes a wound to identity.

In advanced stages, pain, reduced mobility, and fatigue can further limit social participation. Isolation increases. Emotional resilience decreases. Eating behaviors often become more chaotic or more rigid in parallel.
Yet not every story is the same.
I have never had a deeply strained relationship with food. I have had moments of irritation toward my body. I have looked at cellulite and wished it were different. I have cringed at photos. But those moments have usually passed. They have not defined me.
During my surgical period, however, the intense focus on my body disrupted my balance. I developed new insecurities. I wanted more procedures. I struggled to speak kindly to myself. I am grateful that my surgeon refused to “take more” when I asked.
Today, I am back to a place of relative self acceptance. I still have fifteen minute windows of self criticism. They just do not dominate my days.
Other women have entirely different trajectories. Some fight eating disorders long before diagnosis. Some develop them after years of pain and failed dieting. Some live with obesity and lipedema together and carry both the metabolic and social burden.
All of these women are part of the same global community.
The biology and the stress loop
Lipedema is characterized by adipocyte hypertrophy, increased fat cell number, chronic inflammation, and progressive fibrosis. Over time, extracellular matrix remodeling leads to tissue stiffening and pain. In later stages, edema and lymphatic impairment may develop.
Chronic psychological stress interacts with these biological processes. Sustained activation of stress pathways increases cortisol and inflammatory signaling. Inflammatory mediators influence adipose tissue behavior. Pain increases stress. Stress increases inflammation. The loop reinforces itself.
Severe restriction or malnutrition may lead to muscle loss, which can reduce mobility and lymphatic support. Coexisting obesity may increase mechanical load and hypoxia in already vulnerable tissue.
Mind and tissue are not separate systems.
This is why management that focuses only on weight is incomplete.
Moving away from moral hierarchies
We will not move forward if lipedema management becomes a moral hierarchy.
There is no single correct diet. There is no universal protocol. The evidence for many interventions, including ketogenic approaches, remains limited and based on small studies. Some women benefit. Others do not.
What we do know is that eating disorders carry substantial disease burden and increased mortality. Psychological safety matters. Flexibility matters. Social connection matters.
Support should prioritize emotional regulation skills, self compassion, realistic expectations, and individualized care. Multidisciplinary approaches that combine medical management, physiotherapy, nutritional guidance, and psychological support are often most sustainable.
The goal is not extreme weight loss. The goal is functional strength, pain reduction, stable mood, and a life that feels livable.
If someone is struggling with severe depression or a significant eating disorder, that deserves specialized treatment. Stabilization is not a failure. It is responsible care.
LipedemaScience is something you won’t find anywhere else. It’s written by someone with real laboratory science experience, who is also navigating the realities of lipedema management in everyday life. If you want to follow the journey, you’re welcome to join. Read the free posts, and if you want full access, become a paid subscriber and come along from the inside.
For all types of lipedema women
Whether you are underweight and restricting.
Whether you are overweight and exhausted from dieting.
Whether you oscillate between control and loss of control.
Whether you have never struggled with food but struggle deeply with pain.
You are not the same. And you do not have to be.
Lipedema does not define moral worth. Food choices are not character tests.
A sustainable path forward reduces systemic stress, protects mental health, and supports tissue function through realistic, flexible strategies. Compression, lymphatic support, gentle movement, and when appropriate, surgery can improve physical symptoms. Therapy, community, and self compassion can stabilize the emotional terrain.
Self acceptance in this context is not passivity. It is a regulatory strategy. It lowers internal stress. It interrupts shame cycles. It makes consistency possible.
Hundreds of millions of women are navigating this condition, many quietly. The least we can do, as a community, is remove judgment from the conversation.
Living with a chronic disease and an eating disorder is complex. It requires nuance, not slogans. It requires science, but also humanity.
And above all, it requires kindness.
So very very true. I’ve had disordered eating for years but because my lower half never became rail thin, no one noticed, no one paid attention. Even doctors, when I asked for the hundredth time-why is my top half thin but my legs don’t change? Their response “you’ll have to eat less”, so I did. Less and less and less. They were assisting in driving an eating disorder. The penny dropped for me when I remember looking at a salad I had prepared myself and deciding ‘what can I remove from this to eat less?’ I also believe disordered exercising goes hand in hand with this condition. Even today there is still that voice when I am in the gym “just stay a bit longer, do another exercise class”. I wonder how many of us negotiate with ourselves over time spent exercising because the narrative we are conditioned to believe is “you just need to move more”? It’s very difficult to silence that voice in my head even with what I now know I’m living with, but I’m getting there.