
Is Lipedema a disorder of both Fat and Muscle?
A new review explores whether advanced lipedema may involve not only fat tissue expansion, but also a deeper loss of muscle quality and function.

Lipedema has traditionally been understood as a disorder of adipose tissue. The defining features are well known: a disproportionate accumulation of subcutaneous fat, pain, edema, easy bruising, and a striking resistance to conventional weight loss strategies. Yet for many women living with the condition, particularly in more advanced stages, this explanation has always felt incomplete. The experience is not only one of increased volume. It is also one of altered function. Legs that appear strong may feel weak. Movement becomes heavier, less efficient, and more exhausting than expected. Over time, there is a growing sense that something deeper than fat accumulation is shaping the body’s behavior.
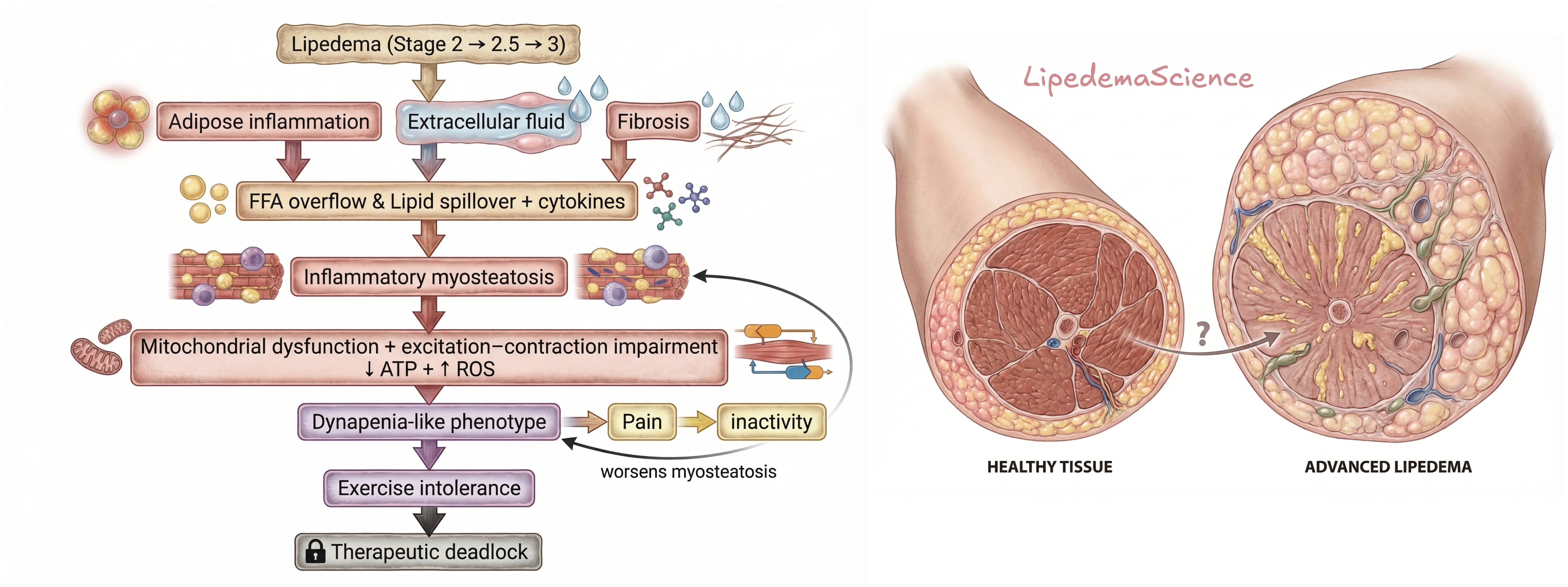
A recent narrative review titled Lipedema and Dynapenia: Inflammatory Myosteatosis as a Mechanistic Link Between Tissue Expansion and Muscle Dysfunction attempts to address this gap. Rather than treating lipedema as a condition confined to adipose tissue, the authors propose a broader, integrated model in which fat and muscle interact in ways that may directly influence physical function. Their central argument is not that adipose tissue is irrelevant, but that in advanced disease, adipose pathology alone may no longer be sufficient to explain the observed decline in strength and mobility. Instead, they suggest that lipedema may evolve into a condition characterized by coupled dysfunction between adipose tissue and skeletal muscle.
The paradox many women recognize
At the core of this hypothesis lies the concept of dynapenia. Dynapenia refers to a reduction in muscle strength that cannot be fully explained by a loss of muscle mass alone. This distinction is critical. In many clinical contexts, weakness is assumed to result from muscle wasting. However, dynapenia challenges that assumption by highlighting that muscle can remain present in terms of size while losing its functional capacity.
In the context of lipedema, this concept resonates deeply with lived experience. Many women notice that their legs are not smaller, not visibly atrophied, and sometimes even described as “strong” by others, yet they feel weaker in everyday life. Walking requires more effort. Climbing stairs becomes disproportionately demanding. There is a sense of inefficiency in movement that is difficult to explain within a purely mechanical model. The review suggests that this mismatch between appearance and function may not be incidental, but rather a defining feature of advanced disease.
Muscle quality rather than muscle size
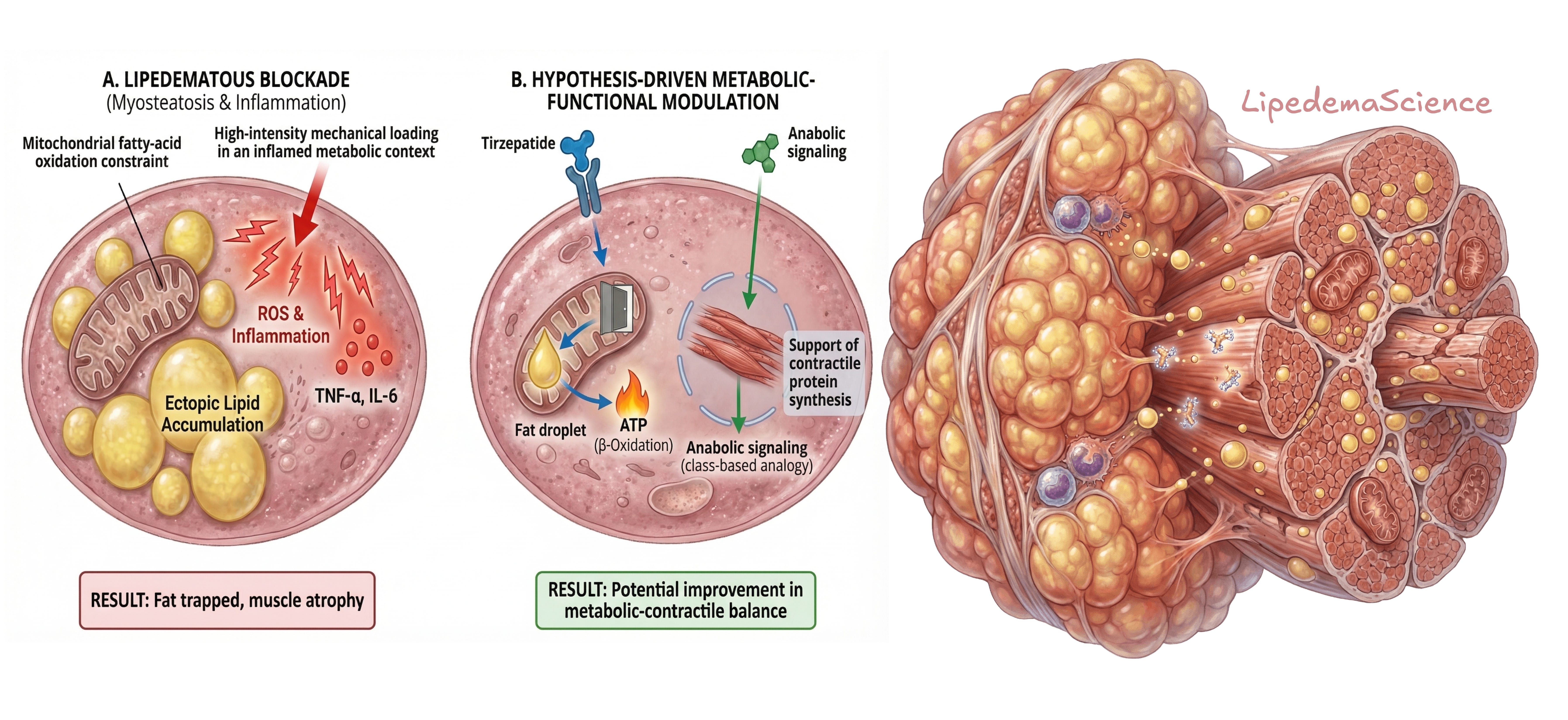
To explain how this might occur, the authors introduce the concept of myosteatosis, defined as the accumulation of fat within and around skeletal muscle. This phenomenon is well documented in other conditions, including aging, obesity, and metabolic disease, where it is associated with reduced muscle quality and impaired physical performance. In this review, myosteatosis is placed within the specific biological context of lipedema.
This is a member-supported platform where every subscriber truly matters. Each person who joins helps expand our collective understanding of lipedema and strengthens a space built on science, experience, and shared insight. If you have not yet subscribed to LipedemaScience, you are warmly invited to support the platform today and be part of a growing, informed community.
The authors propose that chronic inflammation in adipose tissue, combined with microvascular dysfunction, interstitial fluid accumulation, and impaired lipid mobilization, may create conditions that favor ectopic fat deposition within muscle. This is not simply a structural change. It alters the internal environment of the muscle. Mitochondrial function may become less efficient, fatty acid oxidation may be impaired, and oxidative stress may increase. Over time, this can reduce the muscle’s ability to generate force and recover from activity.
This shifts the focus from muscle quantity to muscle quality. It suggests that even when muscle mass appears preserved, the functional capacity of that muscle may be significantly compromised.
The illusion of strength
One of the more subtle but important ideas in the review is the concept of pseudo-hypertrophy. In a healthy physiological context, hypertrophy reflects adaptive growth of muscle in response to load, resulting in increased strength. In lipedema, however, the authors suggest that increased limb volume may not reflect true functional muscle expansion.
Instead, the tissue may consist of a combination of fluid, fibrosis, inflammatory changes, and fat infiltration. From the outside, this can create the impression of substantial mass. Internally, however, the proportion of contractile, functional muscle tissue may be lower than assumed. This helps explain why many women feel that their bodies are misinterpreted. What is seen as strength may in reality be non-functional tissue burden.
A critical transition in disease progression
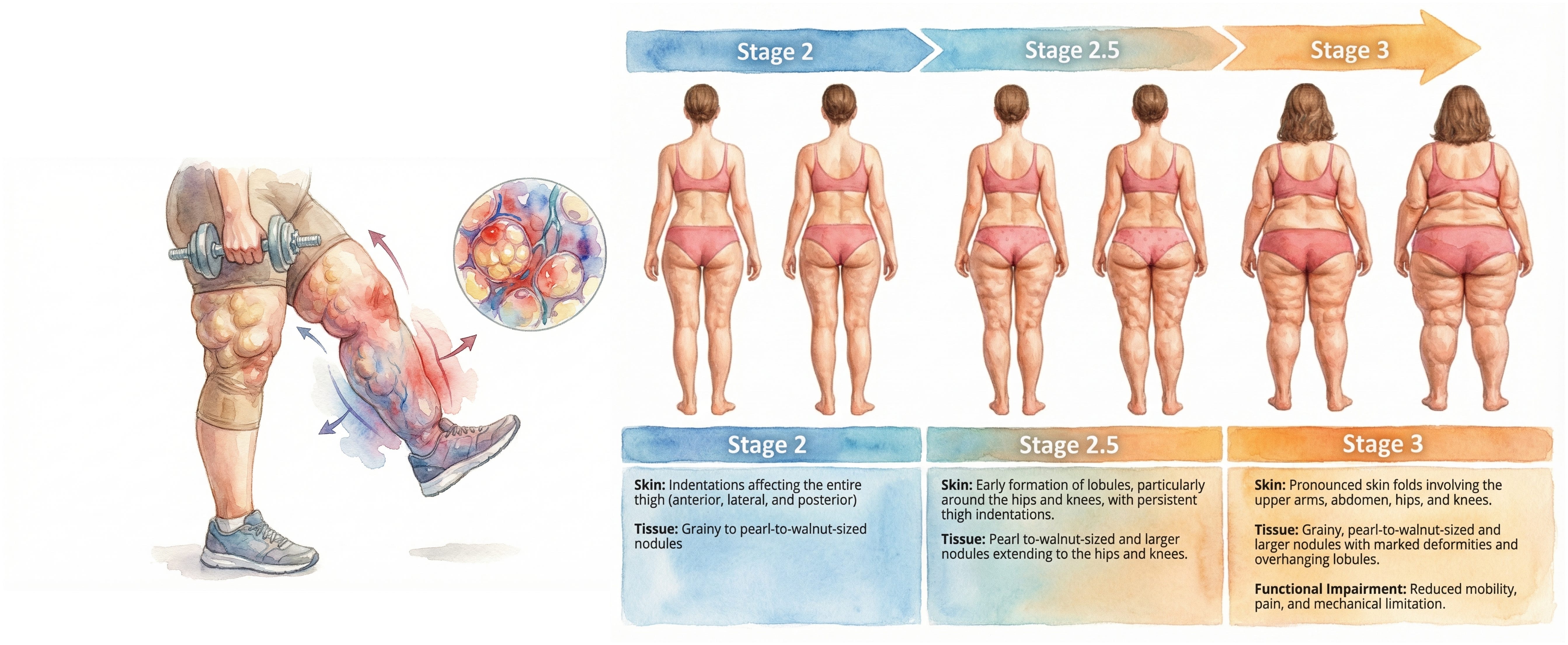
The review places particular emphasis on the transition between Stage 2.5 and Stage 3, describing it as a potential functional turning point. While earlier stages are largely characterized by adipose expansion and structural changes, the authors suggest that functional decline may begin more subtly before becoming clinically obvious.
For women living with lipedema, this is a meaningful insight. It suggests that the feeling of “something changing” in how the body functions may not be imagined or incidental. It may reflect an underlying biological shift that precedes visible disability. By the time Stage 3 is reached, the mismatch between limb size and functional capacity becomes more pronounced, but the process may have been developing for some time.
Why standard measurements fall short
A key reason this phenomenon has been difficult to capture is the reliance on traditional metrics such as BMI. BMI does not distinguish between fat, muscle, fluid, or fibrotic tissue, and therefore cannot reflect qualitative changes in tissue composition. Even body composition tools can be misleading in the presence of edema and inflammation.
This creates a gap between measurement and experience. Women may be told that their muscle mass is normal or even elevated, while they themselves feel a clear decline in strength and endurance. The review highlights the need for more precise approaches that assess muscle quality rather than relying solely on size or weight-based metrics.
Inflammation and metabolic environment
Inflammation is a central component of the proposed model. The authors draw on evidence showing that chronic low-grade inflammation can impair muscle strength independently of muscle mass. In lipedema, adipose tissue is not passive. It may actively contribute to an inflammatory environment that affects neighboring tissues, including muscle.
At the same time, metabolic flexibility may be reduced. If the muscle becomes less capable of efficiently oxidizing fatty acids, energy production becomes less adaptable. This can lead to increased oxidative stress and reduced contractile efficiency. In this context, muscle dysfunction is not simply mechanical. It is embedded in a broader metabolic and inflammatory network.
The exercise paradox
This model has important implications for how we think about exercise in lipedema. In most populations, resistance training is essential for maintaining and improving muscle strength. However, the review suggests that in advanced lipedema, the tissue environment may not tolerate mechanical loading in the same way.
Increased inflammation, edema, and pain may limit the ability to train effectively. Recovery may be impaired. What is typically a beneficial stimulus can become a source of symptom exacerbation. This creates a paradox in which the body requires load to maintain strength, yet becomes increasingly unable to tolerate that load.
For many women, this is not a theoretical concept. It reflects a lived reality. The experience of trying to exercise, only to feel worse afterward, is common. This review offers a biological framework for understanding why that might happen.
A cycle that reinforces itself
The authors describe a self-reinforcing cycle in which inflammation, fat infiltration in muscle, reduced muscle quality, pain, and decreased activity interact over time. As movement becomes more difficult, activity levels decline. As activity declines, muscle function deteriorates further. This, in turn, makes movement even more demanding.
This perspective is important because it shifts the narrative away from individual responsibility. Reduced activity is not framed as a lack of effort or discipline, but as a consequence of a biological environment that makes movement increasingly challenging.
What this study adds, and what it does not prove
It is important to be clear about what this study represents. It is a narrative, hypothesis-generating review. It does not provide direct experimental evidence that inflammatory myosteatosis occurs in lipedema. Much of the supporting evidence comes from related fields, and while the proposed mechanisms are plausible, they have not yet been directly confirmed in this specific condition.
There are significant gaps in the research. We lack muscle biopsy studies in lipedema. Longitudinal imaging of muscle quality across disease stages is limited. The timing and progression of these changes remain unclear. The authors themselves emphasize the need for further investigation.
Why this matters
Despite these limitations, the study offers something valuable. It provides a framework that aligns more closely with the lived experience of many women with lipedema. It suggests that functional decline may have a biological basis that extends beyond fat accumulation alone.
It also invites a more nuanced understanding of the condition. Instead of viewing lipedema solely as a disorder of adipose tissue, it encourages us to consider how fat, muscle, inflammation, and metabolism interact over time.
Final reflection
For many years, the dominant question in lipedema has been how much fat is present. This review suggests that an equally important question may be how well the tissue functions.
For women living with lipedema, this shift matters. It validates the experience of feeling weaker despite unchanged or increased limb size. It acknowledges that the body may be changing in ways that are not immediately visible, but are deeply felt.
We do not yet have definitive answers. But this model offers a direction. It suggests that understanding lipedema may require looking beyond volume alone and paying closer attention to muscle quality, metabolic health, and the biological environment in which the disease develops.
And perhaps most importantly, it reminds us that when the body feels different, even if it looks the same, there is often a reason worth investigating.
Lipedema and Dynapenia: Inflammatory Myosteatosis as a Mechanistic Link Between Tissue Expansion and Muscle Dysfunction (DOI: 10.3390/ijms27052319)
Should people with lipedema still exercise, specifically those that feel they need more rest days than the average person? Or someone in later stages? Can progressive overload actually cause more harm than good for the muscles for someone with lipedema if the muscles may not be recovering well? Seems like something the individual might not even recognize till it’s too late. Obviously I’m not talking about over exerting yourself, or over doing it, but trying to build muscles in general. .This disease just seems like an end all. Really discouraging every corner you turn.