
Hormones and Lipedema: What a New Systematic Review Tells Us
Impact of hormones on lipedema development: a systematic literature review from January 2026.

On January 8, 2026, a new systematic review was published in Archives of Gynecology and Obstetrics. It examines something many of you have sensed in your own bodies long before science caught up: lipedema is deeply connected to hormones.
Not as a vague association. Not as a side note. But as a central driver of how the disease develops, progresses, and resists conventional treatment.
Today is January 26. That means this paper is still very new. It also means we now have one of the most comprehensive summaries to date of how hormones may shape lipedema at a biological level. This article is about what the review found, but more importantly, what it means for you if you live with lipedema.
Why this review matters
Lipedema has long been misunderstood. It has been confused with obesity. It has been dismissed as lifestyle-related. It has been framed as a cosmetic problem rather than a medical one. A major reason for this is that we still lack clear diagnostic markers and a widely accepted disease model.
This review directly challenges that gap.
The authors systematically examined the existing scientific literature to understand how hormones influence lipedema development. After screening more than 100 publications, only 15 met the criteria for inclusion. That number may sound small, but it reflects the reality of lipedema research: this is still an early field, and high-quality mechanistic studies are rare.
Despite that limitation, a consistent pattern emerged.
Across different study types, tissues, and hypotheses, the same message appeared again and again: lipedema behaves like a hormonally driven disorder of adipose tissue, not like simple fat accumulation.
Lipedema and hormonal life transitions
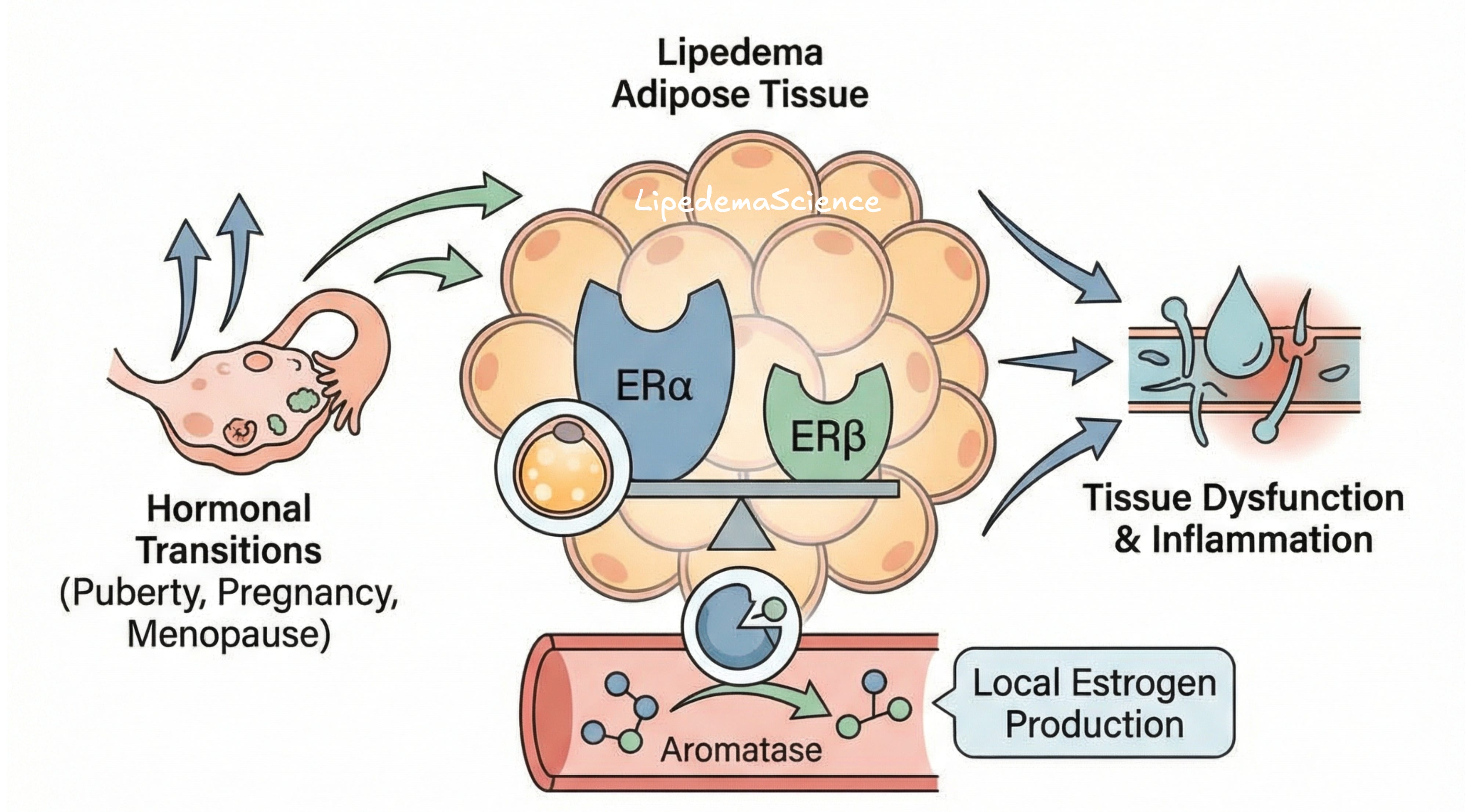
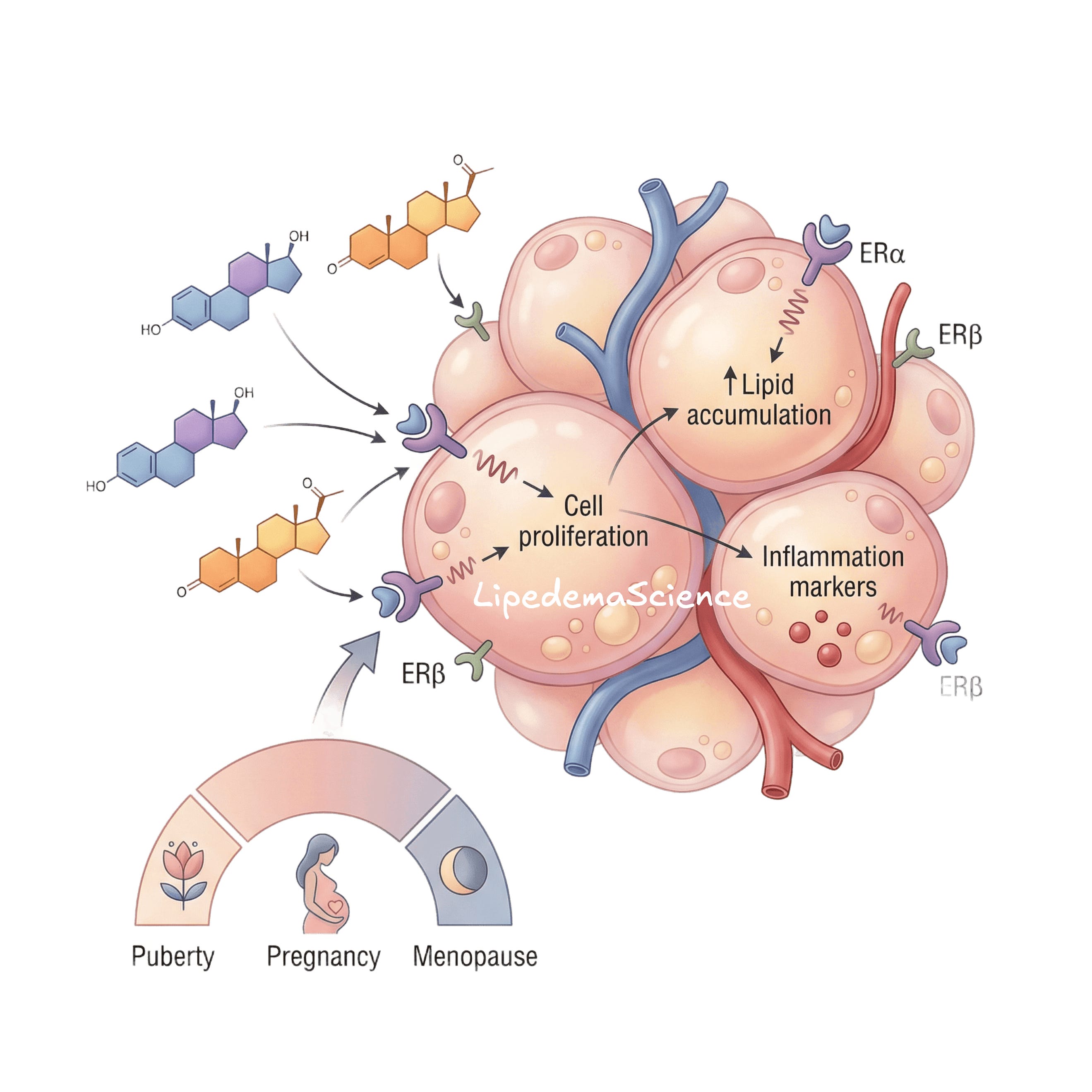
One of the strongest observations, both clinically and scientifically, is that lipedema often appears or worsens during hormonal transitions.
Puberty
Pregnancy
Menopause
This is not coincidental.
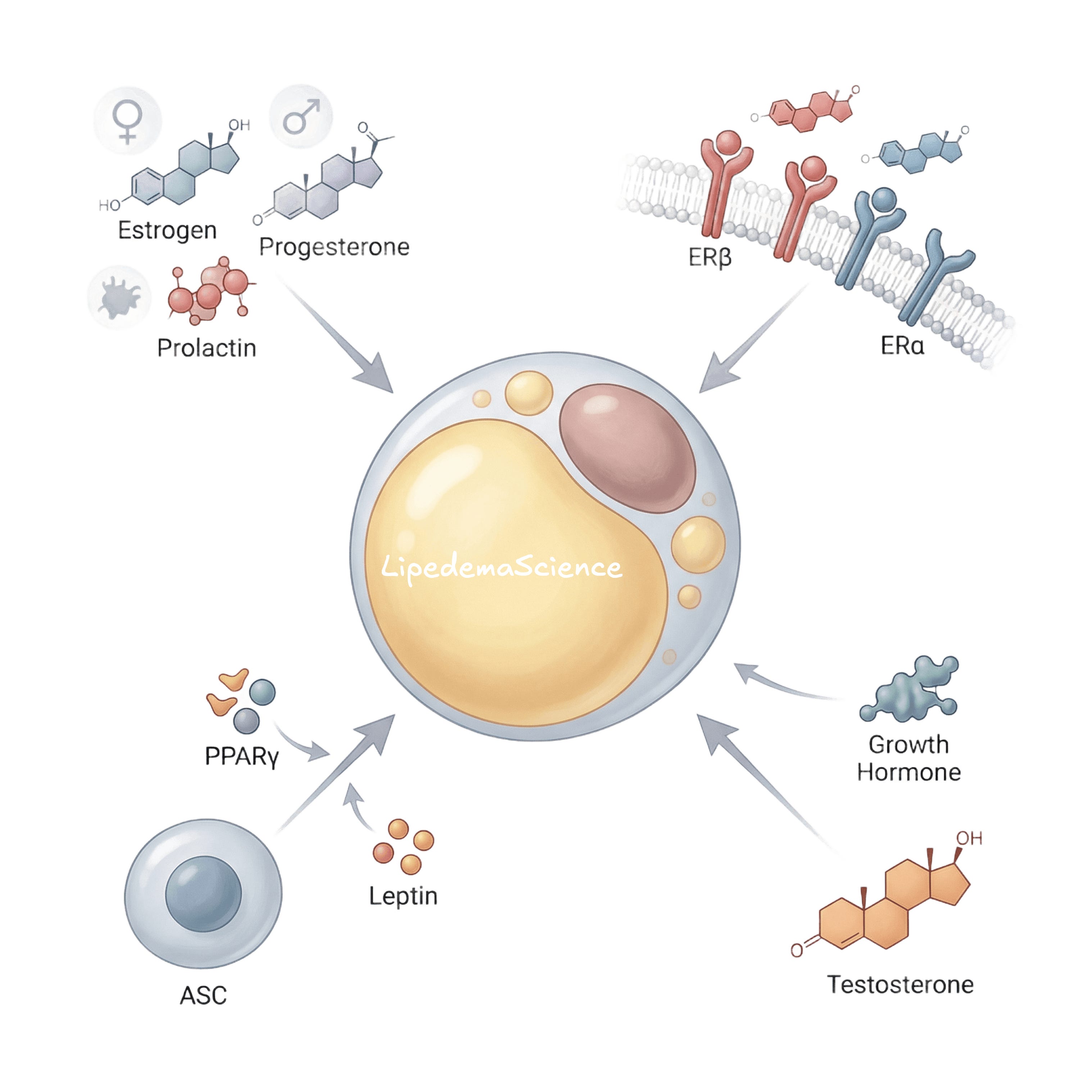
The review emphasizes that estrogen and progesterone shape where fat is stored, how fat cells grow, and whether fat can be broken down. These hormones are meant to support reproduction and energy storage in women. In lipedema, those same mechanisms appear to become dysregulated.
Several studies describe lipedema as resembling a “pseudo-pregnancy” hormonal state. Not because women with lipedema are pregnant, but because the tissue behaves as if it is constantly receiving signals to store fat, retain fluid, and avoid lipolysis.
That framing matters. It helps explain why calorie restriction and exercise often fail to change lipedema tissue, even when overall weight changes elsewhere in the body.
Estrogen is central, but not simple
Estrogen is not one hormone with one effect. It works through receptors, mainly ERα and ERβ, and those receptors behave differently depending on tissue type, location, and balance.
One of the most consistent findings across the reviewed studies is altered estrogen receptor signaling in lipedema tissue.
In simple terms:
The ratio between ERα and ERβ appears shifted in lipedema fat, especially in the thighs and hips.
Why does that matter?
Because ERα tends to promote fat storage, glucose uptake, angiogenesis, and reduced fat breakdown. ERβ, in contrast, is more closely linked to mitochondrial function and metabolic flexibility. When this balance is disturbed, adipose tissue becomes biased toward expansion rather than turnover.
This altered receptor pattern may explain several hallmark features of lipedema.
Why fat accumulates disproportionately in the legs and arms
Why that fat is resistant to weight loss
Why the usual menopausal shift toward abdominal fat often does not occur in lipedema
Importantly, this is not the same receptor pattern seen in obesity. That distinction is critical.

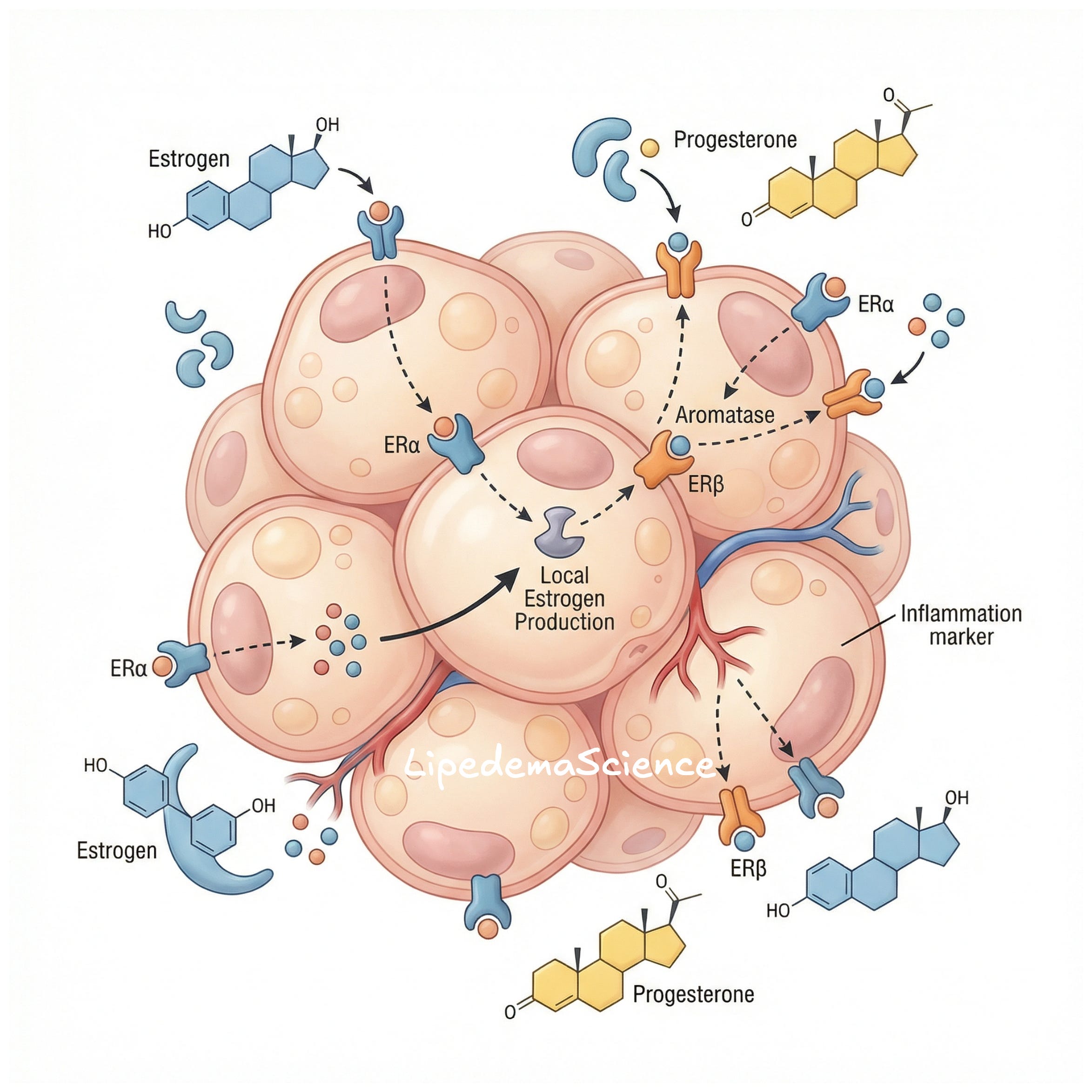
Local estrogen production inside fat tissue
Another key insight is that estrogen in lipedema may not only come from the ovaries or circulation.
Fat tissue itself can produce estrogen through aromatase activity. Several studies included in the review show increased aromatase expression in lipedema adipose tissue, particularly in perivascular and stem-cell-like populations.
This means lipedema tissue may create its own hormonal microenvironment.
Local estrogen production can amplify fat growth, vascular changes, and inflammation even when blood hormone levels appear normal. This may help explain why standard hormone tests often fail to reflect what is happening inside affected tissue.
It also means that lipedema cannot be understood by blood markers alone.
Adipose stem cells and metabolic dysfunction
The review highlights growing evidence that lipedema is not just about mature fat cells, but about how new fat cells are formed.
Adipose-derived stem cells from lipedema tissue behave differently from those in unaffected fat.
Some studies show exaggerated adipogenic potential in the thighs. Others show impaired differentiation but altered signaling. At first glance, this looks contradictory. In reality, it suggests that lipedema fat is metabolically abnormal and context-dependent.
What is consistent is that key regulators like leptin and PPARγ are dysregulated. These molecules control fat cell differentiation, size, and energy handling. Their interaction with estrogen signaling appears to be a major axis in lipedema biology.
This matters because it reframes lipedema as a disorder of tissue programming, not willpower.
Genetics and hormone metabolism
One of the most striking findings discussed in the review involves a mutation in the AKR1C1 gene.
This gene is involved in progesterone metabolism. In one family with inherited lipedema, a loss-of-function mutation impaired progesterone inactivation. The result was increased fat accumulation and altered lipid metabolism.
This does not mean lipedema is always genetic or always caused by this mutation. But it does show that hormone metabolism genes can directly influence lipedema development.
The review also discusses other structural and signaling proteins, such as caveolin-1, that link estrogen signaling to vascular and connective tissue changes.
Together, these findings support the idea that lipedema may be hormonally sensitive and, in some cases, inherited in a sex-limited way.
What this review does not claim
It is important to be clear.
This review does not prove causation.
It does not offer a diagnostic blood test.
It does not provide a ready-made treatment.
Most included studies are observational or preclinical. Sample sizes are small. Hormonal confounders like contraceptive use and menopausal status are inconsistently reported.
But that does not make the findings weak. It makes them early.
What matters is consistency. And across different approaches, estrogen receptor dysregulation appears again and again as a core feature.
Why this matters for people with lipedema
First, it reinforces that lipedema is not obesity.
The biology is different. The tissue behavior is different. The response to weight loss is different. This matters for stigma, self-blame, and medical recognition.
Second, it explains why symptoms often worsen during hormonal transitions. These are not failures of management. They reflect real biological sensitivity.
Third, it points toward future diagnostics that go beyond BMI and visual inspection. Multi-marker panels combining hormones, metabolic signals, and genetics are a logical next step.
Finally, it opens the door to targeted therapies. Not blanket hormone manipulation, but careful modulation of receptor signaling, tissue metabolism, and microenvironmental factors.
That work is not here yet. But the foundation is becoming clearer.
A necessary shift in how lipedema is understood
Perhaps the most important contribution of this review is conceptual.
It argues that lipedema should be recognized as a hormonally influenced adipose tissue disorder, distinct from obesity.
That shift is not semantic. It affects research funding, clinical training, diagnostic criteria, and how patients are treated and believed.
Science does not move fast. But it does move forward.
This review is one step in that direction.
And for many of you, it finally puts words and mechanisms to what your body has been telling you for years.
Impact of hormones on lipedema development: a systematic literature review (DOI: 10.1007/s00404-026-08318-1)
I could cry from reading this. I have endometriosis which also creates extra estrogen, and ive always blamed myself and not trying hard enough but once i got on a glp1 and hrt, eating well and doing Pilates, and still had the fat, I knew it wasn’t my fault. Thank you for your hard work in gathering these studies and sharing them. It’s healing. I will also share on my platform!
Dette er veldig spennende! Og med bakgrunn i dette står eg enda stødigere i mitt standpunkt på å ikkje tilføre kroppen meir hormoner, sjølv om eg kanskje hadde trengt det for ein smidigere kvardag gjennom overgangsalderen. Men den risikoen tør eg ikkje ta 💔🙈🍀🍀