
Do I Still Need Lymphatic Care After Lipedema Surgery?
A personal reflection on compression, water, dry brushing, movement, and maintenance.

Since my lipedema surgeries, I have found myself thinking differently about lymphatic care.
During the years around surgery, the role of lymphatic support felt relatively clear to me. I used compression garments. I used a lymphatic press. I went to manual lymphatic drainage with a physiotherapist. These were not small additions to my life at the time. They were part of the structure around surgery, recovery and tissue healing. My body was swollen, sensitive and changing, and I wanted to give it every reasonable form of support I could.
That phase had its own logic. The phase I am in now feels different.
I am several years post-surgical, and I would describe my current situation as maintenance rather than active recovery. I travel frequently, and my life is not organised around being in one place with access to all the tools I used before. I cannot bring a lymphatic press with me everywhere. I cannot always plan physiotherapy appointments. I do not want my health routine to become so elaborate that it only works under perfect conditions.
At the same time, I notice a familiar question returning in the background:
am I doing enough for my lymphatic system?
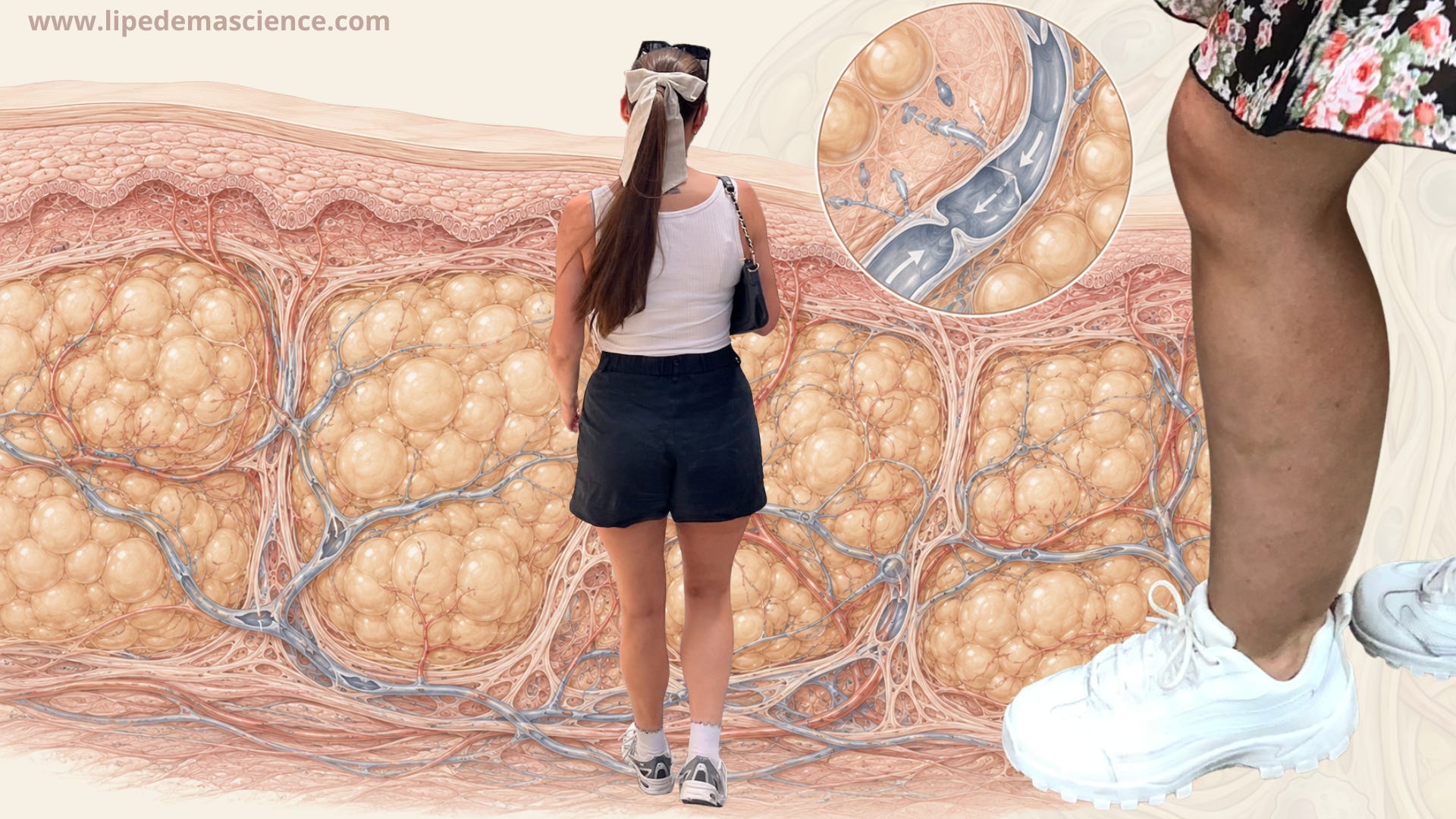
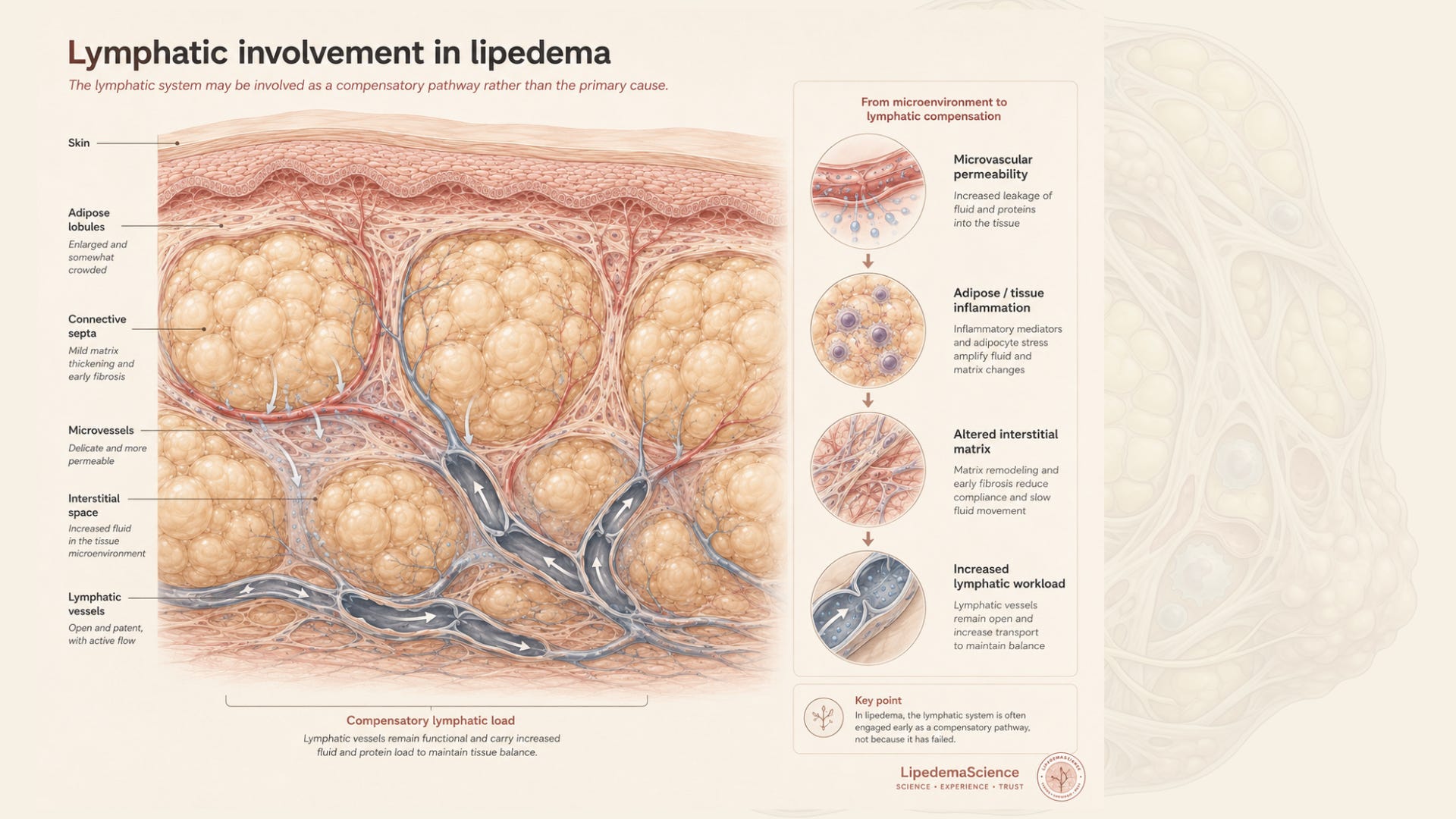
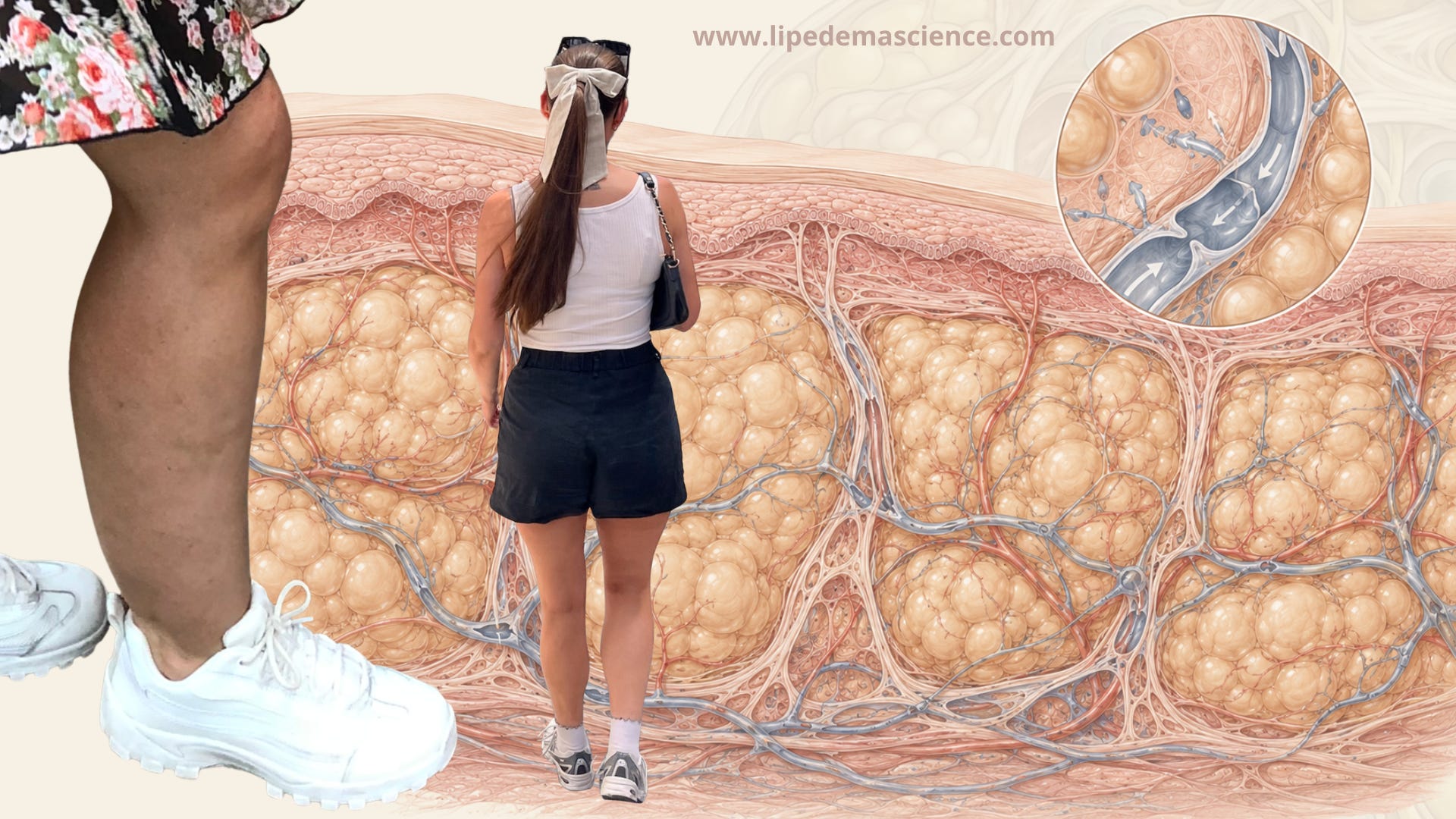
It is a difficult question, because the lymphatic system occupies a strange place in lipedema. It is often mentioned in patient communities, treatment protocols and commercial messaging, but the scientific picture is still more nuanced than many explanations suggest. Lipedema is not simply lymphedema. The legs may feel swollen, heavy and pressurised, but that does not necessarily mean the primary problem is failed lymphatic drainage. Several studies suggest that pure lipedema is not characterised by the same fluid accumulation seen in lymphedema, and some imaging studies indicate that the lymphatic vessels may still be functioning, at least in earlier stages.
Subscribe to LipedemaScience if you want evidence-based writing about lipedema without oversimplified advice or wellness claims. I look at the research, the limitations, and the practical questions patients are left with. The goal is to make lipedema science easier to understand and use in real life.
That does not mean the lymphatics are irrelevant. It means the question is more complicated.
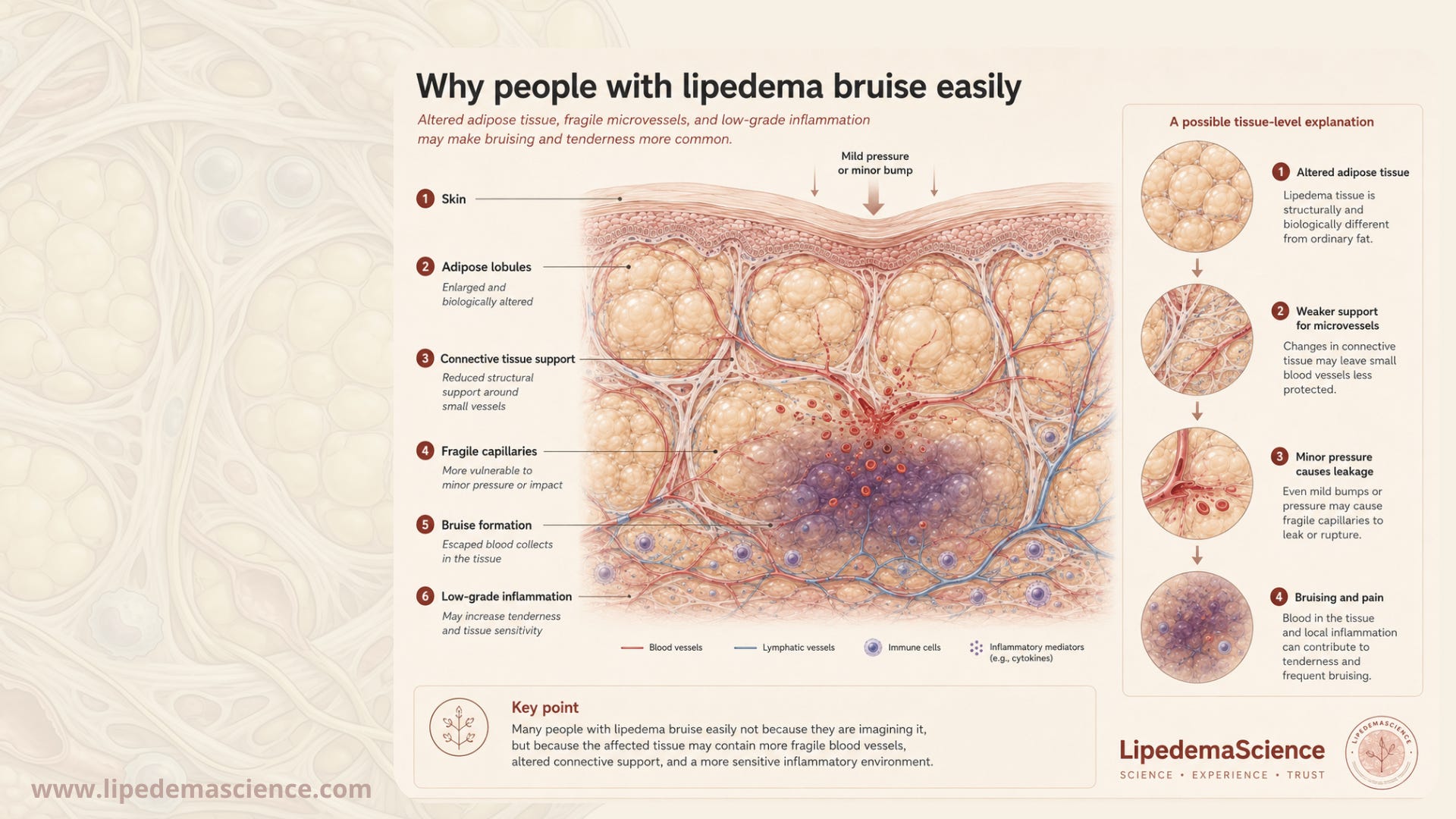
One model I keep returning to is that the lymphatic system may not be the first thing that breaks. It may be the system that is asked to compensate. If the small blood vessels in lipedema tissue are more fragile or more permeable, if the fat tissue is inflamed, if the interstitial matrix becomes more fibrotic or altered, then the lymphatics may be handed more work than they would receive in a normal limb. In that case, the lymphatic system is involved, but perhaps not as the original cause. It may be carrying part of the burden created by the adipose and microvascular environment.
This distinction matters, because it changes how I think about treatment.
If lymphatic support mainly helps symptoms, then it may still be valuable. Compression may reduce heaviness, pain, bruising or swelling sensations. Pneumatic compression may be useful when fluid or pressure builds up. Manual lymphatic drainage may feel calming and supportive, especially in periods of recovery or flare. Water may offer a gentle form of hydrostatic compression that also supports movement and circulation. These things may improve comfort and quality of life.
But are they modifying the disease itself? Are they changing the altered fat tissue? Are they reducing fibrosis? Are they preventing progression? Are they protecting the lymphatic system over decades? I do not think we can answer those questions with confidence yet.
This is where I find myself with more questions than conclusions.
In my own life, I have shifted my focus toward the things I can sustain consistently: sleep, stress regulation, less alcohol, nutrient-dense food, running and strength training. These do not look like classic lymphatic treatments, but I increasingly wonder whether they may be central to maintenance. Muscle contraction supports venous and lymphatic return. Strength protects function. Cardiovascular fitness supports circulation. Sleep and stress regulation influence inflammation, recovery and hormonal signalling. Food quality affects metabolic health and perhaps the inflammatory environment in which the tissue exists.
None of this is specific enough to call it a lipedema treatment in the narrow sense. But perhaps maintenance after surgery is not only about targeting the lymphatic system directly. Perhaps it is also about supporting the broader biological environment that the lymphatic system has to operate within.
That is something I want to understand better.
I also try to be in water as often as I can. This is partly because it feels good, but also because the mechanism makes sense to me. Immersion creates external pressure around the limbs. The deeper the body is submerged, the greater the hydrostatic pressure. Combined with movement, water can support circulation, muscle activity and fluid return in a way that feels far less burdensome than compression garments. For someone who travels, water is also more accessible than many devices. A pool, the sea or even gentle movement in water can become a form of care that does not require carrying equipment.
Recently, I also bought a dry brush.
I did not buy it because I believe it will cure lipedema. I do not expect it to break down fat tissue or meaningfully change the disease. I bought it because I was curious. It is simple, portable and inexpensive, and I wanted to see whether gentle skin stimulation might feel beneficial in my body.
But dry brushing is also exactly the type of intervention that makes me cautious.
It is often described as “stimulating the lymphatic system,” but I have not seen good evidence that it improves lipedema symptoms, reduces limb volume or changes lymphatic function. The proposed mechanism is not impossible. The superficial lymphatics sit close to the skin, and mechanical stimulation may plausibly create some sensory or local circulatory effect. But plausible is not the same as proven. This is where the boundary between physiological possibility and wellness marketing becomes difficult to navigate.
I do not want to dismiss every practice simply because the evidence is incomplete. Many parts of conservative care in lipedema are under-researched, and lived experience can sometimes point toward questions that science has not yet studied properly. At the same time, I do not want to present low-evidence practices as if they have stronger support than they do.
So I am treating dry brushing as a small personal experiment, not as a medical intervention.
If it feels calming, improves my relationship with my skin, or gives me a few minutes of quiet body awareness, that may be reason enough to continue. If it irritates my skin or becomes another task on an already long list of things women with lipedema are told to do, I will stop.
This, I think, is one of the hardest parts of living with lipedema in the current evidence landscape. There are many recommendations, but not always enough data to separate what is essential, what is optional, what is helpful for some, and what is mostly commercial enthusiasm. The field contains real science, clinical experience, patient knowledge and marketing claims, often mixed together in the same conversation.
I find myself asking more and more questions..
How much lymphatic support is actually needed after surgery?
Does that need change depending on whether someone has pure lipedema or lipolymphedema?
Are some people more dependent on compression and drainage than others because of venous disease, fibrosis, stage, surgery history or inflammation?
Can strength training and aquatic exercise reduce the need for more passive lymphatic treatments?
Does the lymphatic system recover some capacity after the fat load is reduced surgically?
Could certain maintenance routines protect against secondary lymphatic overload, or is that still an assumption?
And how do we design care plans that women can actually live with for decades?
I do not have clear answers to these questions. But I think they are important questions, because they move the conversation away from guilt and toward individualised care.
Subscribe to LipedemaScience if you want a more critical look at what we actually know about lipedema. I write about research, treatment claims, patient experience, and the many questions that are still unanswered. The goal is not to give perfect answers, but to separate evidence from assumptions.
My own maintenance routine is not perfect, and perhaps that is the point. It is not designed to be perfect. It is designed to be livable. I use compression when it makes sense, especially during flights or situations where I know my legs may react. I prioritise movement, strength, food quality, sleep and stress regulation. I seek water when I can. I remain open to tools like dry brushing, but I hold them lightly.
I am still trying to understand what my body needs now compared with what it needed during surgery recovery.
I am also curious how other women experience this shift.
For those who have had lipedema surgery, did your need for compression, manual drainage or pneumatic compression change over time?
Did you feel able to reduce some of these supports, or did you continue needing them?
Have you found water, strength training or other forms of movement to be enough for maintenance?
Has dry brushing done anything noticeable for you, or does it feel more like a pleasant ritual than a treatment?
I would especially like to hear from people in different stages: those with early lipedema, those who are post-surgical, and those who have lipolymphedema or clear fluid accumulation. My suspicion is that “lymphatic care” is not one thing, and that the right level of support may depend heavily on the person, the stage, the tissue, the comorbidities and the phase of life.
For now, I am trying to stay in the space between certainty and dismissal.
I do not believe my lymphatic system is simply broken. I also do not believe it is irrelevant. I think it may be carrying part of the load created by a more complex tissue environment involving fat, vessels, inflammation, fibrosis and mechanical pressure. That is the part I want to learn more about.
And perhaps this is where I currently land: maintenance after surgery is not necessarily about doing every lymphatic intervention forever. It may be about understanding which forms of support still give something back, which ones belong to a previous phase, and which ones are simply not worth the energy anymore.
That answer will probably not be the same for everyone. And I think that is exactly why we need more honest conversations about it.