
Can Exercise Improve Life with Lipedema? Inside Norway’s LipidEx Research Programme
A closer look at Norway’s LipidEx research programme and what it may teach us about pain, physical capacity, quality of life and the role of exercise in lipedema care.

For many women with lipedema, exercise is associated with a complicated mixture of hope, frustration and uncertainty. We are often told that physical activity is important, yet the advice is rarely specific enough to account for the realities of living with painful, heavy and sometimes highly sensitive tissue. Some women find that running, strength training or cycling improves their function and well-being. Others experience cramping, increased pain, swelling or prolonged fatigue after demanding sessions. At the same time, many have spent years exercising without seeing the expected changes in the size or shape of their legs and arms, which can reinforce the mistaken belief that they have somehow failed.
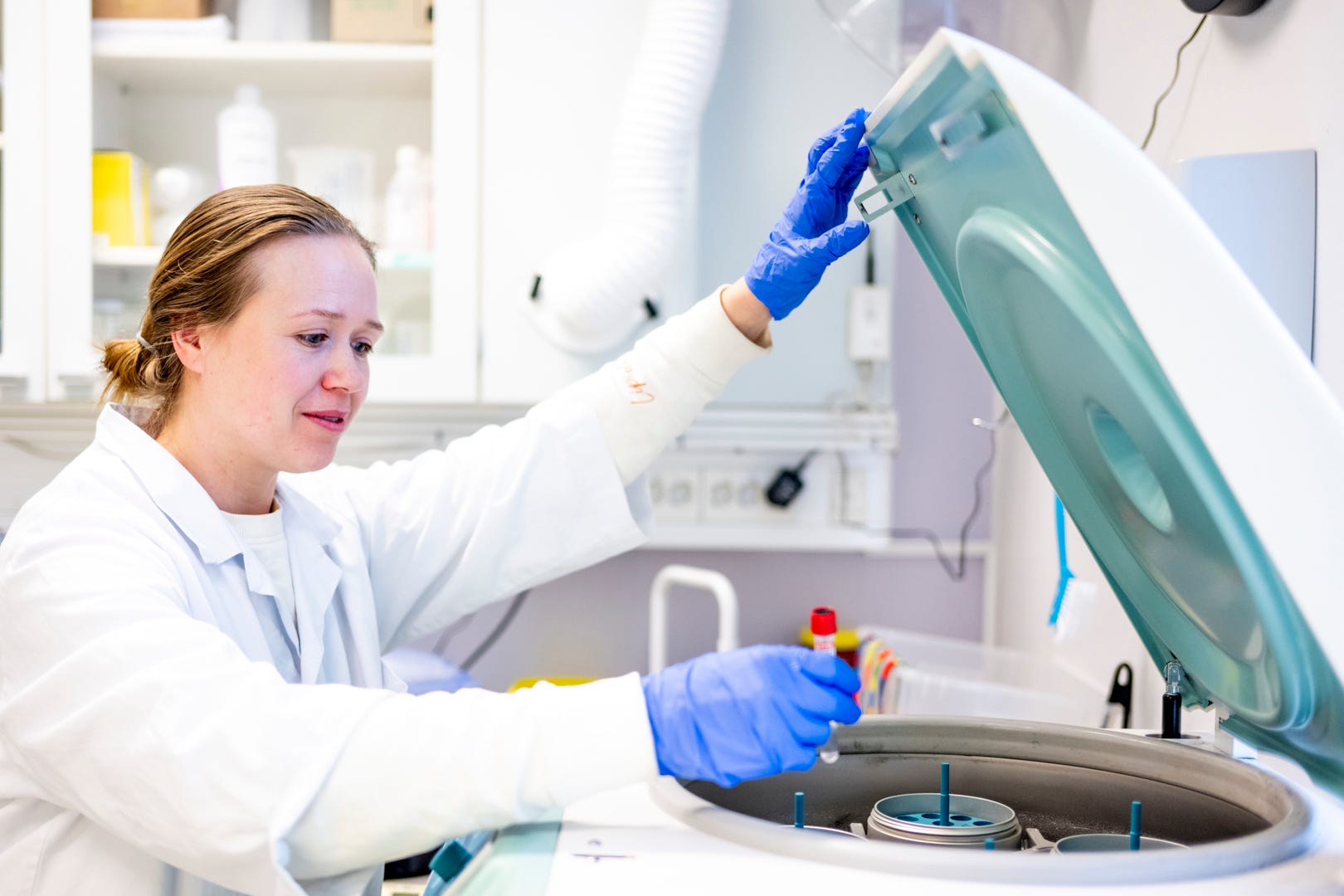
This article highlights the work of Dr. Julie Caroline Sæther, Postdoctoral Researcher at the Department of Circulation and Medical Imaging, Faculty of Medicine and Health Sciences at NTNU, located at St. Olavs Hospital in Trondheim, Norway. With a background in Human Movement Science, Exercise Physiology and Medicine and Health Sciences, her research brings together clinical exercise science, cardiovascular health and biomarker analysis in the study of lipedema.
Special thanks also go to photographer Jan Inge Haga, whose photographs from the LipidEx research project help document the people, the training environment and the important work taking place in Trondheim.
Most importantly, this article is dedicated to the women who participated in the studies. By showing up, completing demanding training programmes, undergoing tests and sharing their experiences, they have made a vital contribution to a field in which knowledge is still far too limited. Their participation is helping researchers build a stronger evidence base for women living with lipedema.
This is why exercise research designed specifically for women with lipedema is so important. General knowledge about the benefits of physical activity cannot automatically answer the questions that matter most to this patient group.
Does exercise reduce lipedema-related pain?
Can it improve daily function and quality of life even when the characteristic adipose tissue remains?
Does the tissue itself change in response to training?
Are some forms of exercise more effective or more tolerable than others?
And what biological processes take place in the blood and adipose tissue when women with lipedema improve their cardiovascular fitness?

Researchers at the Norwegian University of Science and Technology, NTNU, and St. Olavs Hospital in Trondheim are now investigating these questions through the LipidEx research programme. The work is being conducted by a multidisciplinary team that includes researchers in exercise physiology, clinical medicine, body composition, adipose tissue biology, analytical chemistry and statistics. Postdoctoral researcher Dr. Julie Caroline Sæther has played a central role in the project alongside Professor Anja Bye and the wider research team.
The significance of their work lies partly in the fact that they are not treating exercise as a generic lifestyle recommendation. They are studying it as a possible therapeutic intervention for a chronic and painful adipose tissue disorder. Their aim is not simply to demonstrate that exercise is beneficial for general health. Instead, they are trying to determine whether a defined training programme can produce measurable changes in pain, quality of life, physical fitness, body composition and biological processes among women diagnosed with lipedema.

The first LipidEx study: high-intensity interval training
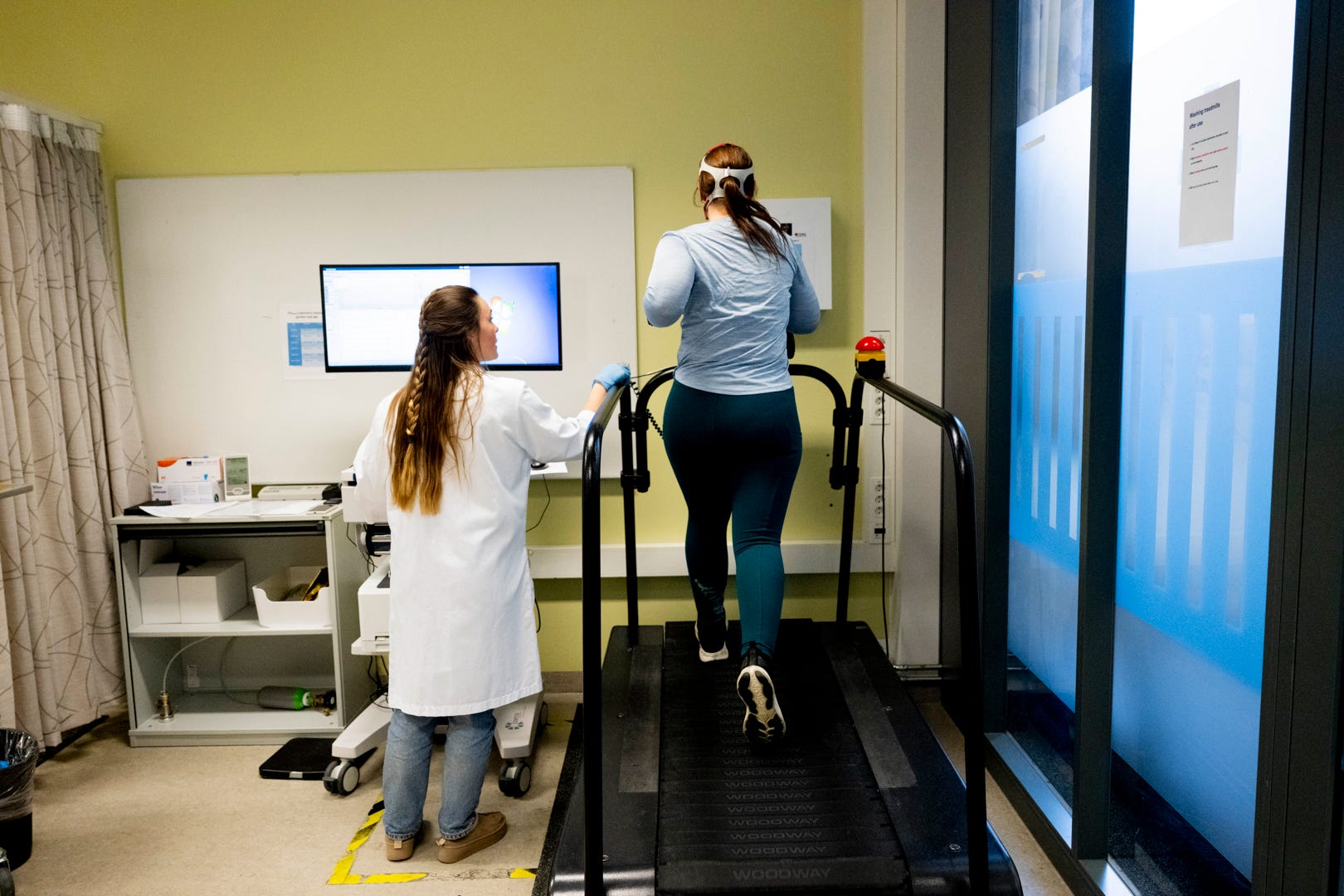
The first study in the programme, often referred to as LipidEx HIIT, examines the effects of twelve weeks of high-intensity interval training. Approximately 60 women between the ages of 18 and 65 with a diagnosis of lipedema were recruited. The participants completed three endurance-training sessions each week. Two sessions were supervised at St. Olavs Hospital, while one was completed independently.
The training included high-intensity intervals based on the Norwegian 4 × 4 model. This involves four periods of four minutes at a high exercise intensity, with active recovery between the intervals. Although the programme was adapted to each participant’s physical capacity, it was intended to be demanding. This was not a study of occasional light movement or general advice to become more active. It was a structured intervention designed to improve cardiovascular fitness and to test how women with lipedema respond to repeated high-intensity exercise over time.

The study uses a randomized controlled design with sequential intervention and control periods. Pain is the primary outcome, while secondary outcomes include quality of life and adipose tissue mass. The research team is also examining physical fitness, body composition, blood pressure and biomarkers in blood and adipose tissue. This allows the researchers to study both the participants’ experiences and the physiological changes that may accompany training.
This combination is particularly valuable in lipedema research. Pain and quality of life cannot be fully understood through laboratory measurements alone, because they are experienced in daily life. At the same time, changes in blood markers, tissue characteristics or body composition cannot be reliably evaluated through personal experience alone. By combining questionnaires, clinical tests, fitness measurements and biological samples, the LipidEx team may be able to connect subjective improvements or difficulties with measurable changes in the body.

The study protocol was made publicly available before the final results were reported. This means that the research questions, outcomes and planned analyses were described in advance. The currently available paper explains what the researchers intend to investigate, but it does not yet provide the final answer as to whether high-intensity interval training reduces lipedema pain or changes the affected tissue.
That distinction is important. The public coverage of the project includes encouraging observations, but these should not be confused with final study results. A participant becoming fitter, progressing from walking to running or feeling a stronger sense of mastery is meaningful, but it does not by itself prove that the intervention has reduced lipedema pain or altered the biology of lipedema tissue. Those conclusions require analysis of the complete dataset and publication of the findings.

What the team has observed during the training period
Even before the final results are available, the project has provided a rare view of how women with lipedema respond to a supervised and demanding exercise intervention. Julie and the research team have described women improving their fitness during the twelve-week period. Some participants initially walked on the treadmill but gradually developed the capacity to run. The researchers also observed a strong social element, with participants encouraging one another, exchanging experiences and creating a sense of community around the training sessions.
This matters because many women with lipedema have a difficult relationship with exercise. Some have been repeatedly told that they simply need to move more or lose weight. Others have learned to distrust their bodies because physical activity has caused pain, heaviness or exhaustion. Entering a supervised research environment where symptoms are taken seriously and exercise is individually adapted may therefore have effects beyond cardiovascular fitness. It can offer a safer setting in which participants can explore their physical capacity without having their symptoms dismissed.

Several participants have described both positive and difficult aspects of the intervention. One woman reported considerable cramping and fatigue during the training period, while also recognising that her physical fitness had improved and that the exercise felt beneficial overall. Another described being in good physical condition and feeling better after extensive training, despite having lived with painful and heavy legs since puberty.

These experiences illustrate why research in this area must avoid overly simple conclusions. Exercise can be demanding and beneficial at the same time. A participant may improve her fitness while still experiencing cramping. She may feel stronger without seeing a major change in the appearance of her legs. She may gain confidence in her body even if her lipedema symptoms do not disappear. Treatment effects in a chronic condition are often multidimensional, and progress cannot always be reduced to a single number.

The team has also been clear that lipedema tissue does not appear to respond to exercise in the same way as ordinary adipose tissue. This is an essential point. The purpose of the study is not to prove that women can exercise away the characteristic fat distribution. Rather, it is to investigate whether exercise can improve symptoms, health and function, and whether it influences the tissue or related biological processes in ways that are not necessarily visible from the outside.
For women with lipedema, this represents a more meaningful understanding of exercise. A training intervention should not be judged solely by whether the legs become smaller. It may still be valuable if it improves cardiovascular capacity, muscle function, mobility, confidence, mental health or the ability to participate in everyday life. The relevant question is not only whether exercise removes affected tissue, but whether it helps the person living with that tissue to function and feel better.

Compression was generally not used during the exercise sessions
Compression garments are frequently discussed as part of conservative lipedema management, but their role during different forms of exercise remains insufficiently studied. I therefore asked Julie whether the LipidEx participants used compression while training.
She explained that the women mainly did not wear compression garments during the exercise sessions. Many, and in her impression most of them, used compression at other times in their daily lives.
This practical detail helps us understand the conditions under which the intervention was carried out. The women were not required to complete the supervised high-intensity sessions while wearing compression. However, because many continued using compression outside the training sessions, the study should not be interpreted as a direct comparison between exercising with and without compression.

A study designed to answer that question would need to assign participants to clearly defined groups and standardize compression use. LipidEx HIIT was designed to investigate the effect of the exercise intervention compared with a control period, not to determine whether compression improves exercise outcomes.
Nevertheless, the information may be reassuring for some women. It shows that participants with diagnosed lipedema were able to complete a supervised high-intensity programme without routinely wearing compression during the sessions. This does not mean that the same approach will suit everyone. Symptoms, disease stage, joint health, mobility, lymphatic complications and personal preference will continue to influence what is tolerable for the individual.

The next step: moderate-intensity endurance training
The Norwegian researchers are not stopping with high-intensity intervals. The next study, LipidEx MICT, examines moderate-intensity continuous training. This is an important development because the question is not simply whether exercise can help, but which form of exercise provides the most useful balance between effect, symptom tolerance and long-term sustainability.
The moderate-intensity study is expected to include approximately 38 women with lipedema. Participants will train three times a week for twelve weeks, with two supervised sessions at St. Olavs Hospital and one independent session. They will be randomized to either a training group or a control group. The researchers will investigate pain, quality of life, body composition, physical fitness and biomarkers in blood.
Moderate-intensity continuous training differs from high-intensity interval training because the participant exercises at a steadier and less intense level rather than alternating between very demanding intervals and recovery periods. For some women, this may be easier to tolerate. It may produce fewer episodes of cramping or excessive fatigue and may be more realistic to maintain without close supervision. On the other hand, high-intensity training may produce larger or faster improvements in cardiovascular fitness. These possibilities need to be tested rather than assumed.
By studying both high- and moderate-intensity approaches, the researchers are beginning to address a much more clinically relevant question than whether exercise is broadly “good” for lipedema. They are asking how exercise should be prescribed. This could eventually help healthcare professionals move away from generic advice and towards recommendations based on intensity, frequency, symptoms and individual capacity.
It is also possible that there will not be one universally superior form of exercise. Some women may benefit from high-intensity intervals and enjoy the sense of achievement they provide. Others may respond better to moderate continuous training. Disease severity, pain sensitivity, previous fitness, body weight, joint problems, age and other health conditions may all influence the response. The long-term goal should therefore not necessarily be to identify one perfect programme, but to develop a better basis for individualized exercise guidance.
Why this research is important for women with lipedema
Women with lipedema have often been left to manage exercise through personal experimentation. We learn from our own bodies, from other patients and from practitioners with varying levels of knowledge. Some discover that swimming or walking in water reduces heaviness. Others prefer strength training, cycling, slow jogging or short intervals. Many adapt the intensity according to pain, hormonal changes, heat, stress and recovery. This practical knowledge is valuable, but it cannot replace systematic research.

The LipidEx programme may help clarify whether exercise affects more than general fitness. If the studies find reductions in pain or changes in quality of life, they may support the development of structured exercise as part of conservative treatment. If the researchers identify changes in biomarkers or adipose tissue, this could also contribute to a better understanding of the biological mechanisms involved in lipedema.
Negative or limited findings would also be important. If high-intensity exercise improves fitness but does not reduce pain, women should know that. If moderate training is easier to tolerate but produces similar benefits, that would be clinically useful. If some participants improve substantially while others do not, researchers may be able to investigate which characteristics predict the response.
This is what serious treatment research should do. It should not begin with the assumption that exercise must work because it is healthy in the general population. Nor should it dismiss exercise because lipedema fat is considered resistant to weight loss. It should test specific interventions, measure outcomes that matter to patients and report both benefits and limitations.

Julie’s background also brings useful expertise to this work. She has previously worked with biomarkers, including microRNAs and lipoprotein subfractions, and now conducts women’s health research through the LipidEx and CorFemina projects at NTNU. This combination of exercise research and biomarker experience may help the team explore how clinical changes relate to processes in blood and tissue.
The research environment is also internationally connected. The LipidEx protocol includes German collaborators Tobias Bertsch and Gabriele Erbacher, and the moderate-intensity study lists the Földi Clinic in Germany among its partners. These relationships matter because lipedema research is still a comparatively small field. Stronger international collaboration may make it easier to compare methods, develop common outcome measures and build larger studies in the future.
A more useful way of thinking about exercise
Exercise is sometimes discussed in lipedema communities in absolute terms. It is either presented as essential treatment or dismissed because it cannot remove the abnormal fat. Both positions are too narrow.
Exercise does not need to cure lipedema in order to improve life with the condition. Better cardiovascular fitness may make walking, travelling and working easier. Stronger muscles may support joints and improve mobility. Greater physical capacity may provide more freedom and reduce the secondary consequences of inactivity. Exercise may also improve sleep, mood and confidence, although these outcomes must still be examined specifically in women with lipedema.
At the same time, women should not be blamed if exercise does not change the size or shape of their limbs. Nor should severe pain or fatigue be interpreted as a lack of discipline. A scientifically responsible approach must recognise that the tissue may respond differently, that symptoms vary considerably and that the optimal intensity is still uncertain.

This is what makes the Norwegian work so valuable. Julie and the LipidEx team are creating a research framework in which women with lipedema are not reduced to their body weight or told to exercise without further guidance. Their pain, quality of life and lived experiences are being studied alongside fitness, body composition, blood markers and adipose tissue.
The final results from the high-intensity study will be needed before we can say whether HIIT is an effective treatment for lipedema-related pain. The moderate-intensity study will add another part of the picture. Further research will then be needed to reproduce the findings, examine long-term effects and identify which women benefit most from different approaches.
Even so, the work already represents progress. It acknowledges that exercise in lipedema is a legitimate and complex research question. It recognises that improving life with a chronic disease may involve more than changing the amount of affected tissue. Most importantly, it begins to replace assumptions with evidence.
For a patient community that has spent years navigating contradictory advice, that is an important step forward.
Thank you so much for sharing this information! I hope you will keep us posted on further results from these studies.