
Anti-Inflammatory Food Is Not One Recipe. Especially Not for Lipedema.
Why the lipedema nutrition conversation needs more nuance than a list of “good” and “bad” foods.

I come to this topic with two perspectives that are difficult for me to separate. I live in a body with lipedema, but I have also studied food and the human body from the inside out. My background is in Human Nutrition and Food Science, and part of my research experience involved working with cells in the laboratory, looking at bioactive peptides, intestinal cells, absorption, and inflammatory signaling.

I have seen how a food-derived compound can appear biologically interesting in a controlled cell model, and I have also seen how far that is from saying that a specific food will have the same effect in a living human body. That experience shaped the way I think about “anti-inflammatory food.” It made me both fascinated and cautious. Fascinated, because food really can communicate with biology. Cautious, because the path from a molecule in a lab to symptom relief in a person with lipedema is long, complex, and often misunderstood.
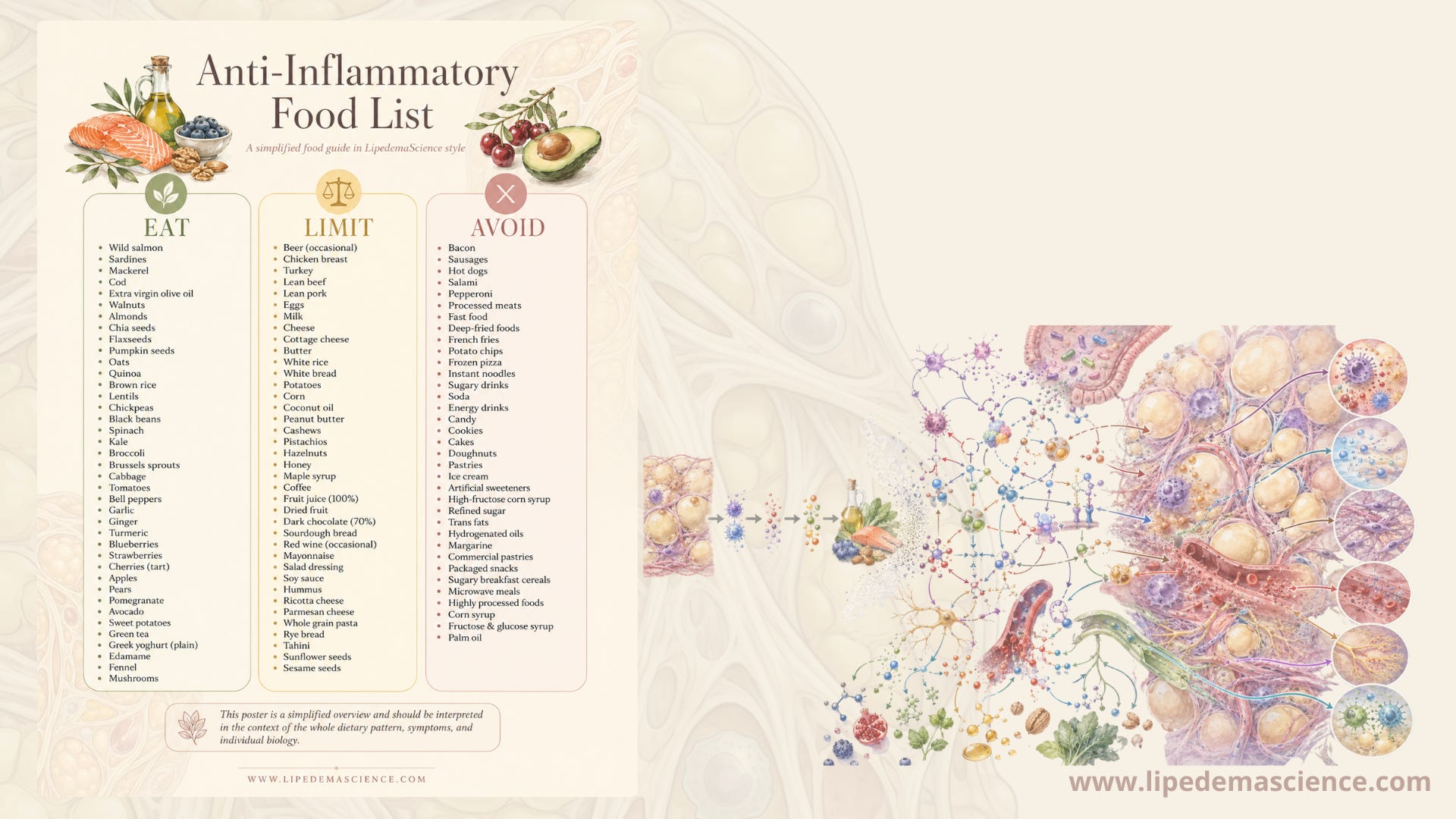
If you have lipedema, you have probably seen the lists.
“Ten anti-inflammatory foods you should eat”
“Avoid these foods to reduce inflammation”
Turmeric, berries, green tea, ginger, olive oil, salmon, walnuts.. They appear everywhere, and they make nutrition sound beautifully simple. Eat from the good list, avoid the bad list, and the body will become calmer.
I understand why that is tempting. When you live with a condition like lipedema, you want something concrete to do. Food is one of the few things we interact with every single day, and it can feel empowering to believe that the right foods might help reduce pain, swelling, heaviness, or that strange tissue pressure many of us know so well.
But this is where I think we need to slow down.
“Anti-inflammatory food” is not a fixed category of foods that works the same way for every person. It is one of the biggest misunderstandings I see in the lipedema community. And when we look at the actual lipedema research, the picture becomes even more interesting.
The popular story often goes something like this: lipedema is an inflammatory disease, therefore you need an anti-inflammatory diet. But the science is not that clean. Lipedema tissue may involve local tissue remodeling, fibrosis, immune cell activity, vascular changes, lymphatic stress and pain. But whether lipedema is primarily a systemic inflammatory condition is still much more unclear than many online discussions suggest.
That does not mean nutrition is irrelevant. It means we need a better question.
Not: which foods are anti-inflammatory for everyone?
But: how does this dietary pattern, in this person, with this biology, affect markers, symptoms, pain, swelling, quality of life and long-term health?
That is a very different conversation.
What inflammation actually is
Inflammation is not automatically bad. It is part of the body’s normal defense and repair system. If you cut your finger and the area becomes red, warm, swollen and tender, that is inflammation doing its job. Immune cells arrive, signals are released, damaged tissue is cleaned up and repair begins.
The problem is not inflammation itself. The problem is when inflammatory signaling becomes long-lasting, low-grade and harder to resolve. This is the type of inflammation people usually mean when they talk about diet and inflammation. It is not the dramatic inflammation of an infected wound. It is a quieter biological background noise that can interact with metabolism, blood sugar regulation, fat tissue, vascular function, gut health, stress, sleep and immune activity.
But even here, we need to be precise. Inflammation is not one thing. It is a whole language of immune cells, cytokines, hormones, enzymes, tissue signals and repair mechanisms. Two people can both be described as having “inflammation”, but the reasons may be completely different. One person may have inflammation driven by insulin resistance. Another by autoimmune disease. Another by gut barrier dysfunction. Another by stress, poor sleep, infection, obesity, endometriosis or chronic tissue injury.
Already, the idea of one universal anti-inflammatory food list starts to fall apart.
A food does not enter an empty laboratory system. It enters a living body with a history.
Lipedema inflammation is more complicated than the online version
This is where the lipedema-specific research matters.
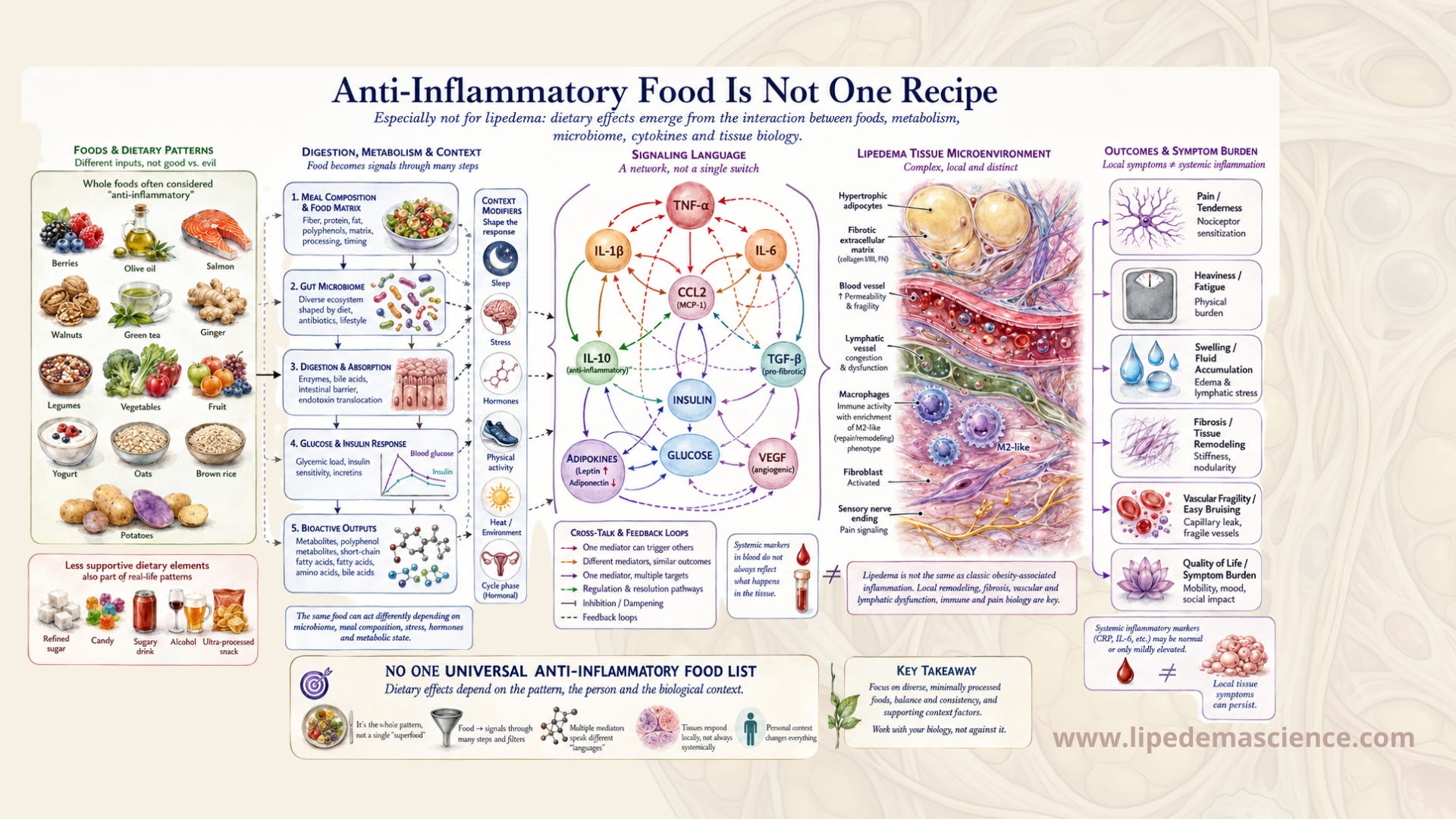
For years, many of us have heard that lipedema is an inflammatory disease. In one sense, that is understandable. Lipedema tissue hurts. It can feel swollen, heavy, bruised, tender and reactive. Several studies describe changes in the affected subcutaneous fat tissue, including fibrosis, adipocyte enlargement, immune cell involvement and tissue remodeling. In later stages, the tissue often becomes more fibrotic and clinically harder. Something is clearly happening in the tissue.
But the immune picture is not the same as in ordinary obesity-related adipose tissue inflammation.
Several recent reviews and tissue studies point toward something surprising: lipedema fat often shows a predominance of M2-like macrophages. Macrophages are immune cells that can take on different roles depending on the tissue environment. Very simplified, M1-like macrophages are often associated with more classic pro-inflammatory immune activation, while M2-like macrophages are often associated with repair, remodeling and more anti-inflammatory signaling.
That does not mean lipedema tissue is “healthy” in the way a person with lipedema experiences it. It hurts. It can be disabling. It can become fibrotic. It can profoundly affect quality of life. But biologically, it may not follow the same inflammatory pattern we see in typical obesity-associated metabolic disease.

Some researchers have even suggested that lipedema may represent a kind of metabolically protected subcutaneous fat expansion, at least in some patients and stages. A population-based study using a lipedema-like body phenotype found lower insulin resistance and a lower neutrophil-to-lymphocyte ratio compared with controls. That does not prove that all clinically diagnosed lipedema is metabolically protective, and it does not erase the lived symptoms of the disease. But it does challenge the simplistic claim that lipedema automatically equals systemic inflammation.
This matters because the popular nutrition logic depends on a very simple chain:
lipedema equals inflammation
inflammation is bad
anti-inflammatory foods reduce inflammation
therefore everyone with lipedema should eat the same anti-inflammatory foods
The research does not support such a straight line.
A more accurate statement would be this: lipedema involves abnormal adipose tissue biology, local tissue changes, immune activity and fibrosis, and some dietary patterns may influence systemic inflammatory markers. But the exact role of inflammation in lipedema is still unresolved, and reducing a blood marker is not the same as reducing pain, swelling or disease burden. That distinction is important.

Where the idea of “anti-inflammatory foods” comes from
When someone says a food is anti-inflammatory, it sounds like a settled fact. But when you look more closely at where much of this knowledge comes from, the picture becomes more complicated.
A lot of anti-inflammatory food research begins in cells, animals or supplement studies. Scientists may take immune cells in a dish, expose them to a purified compound from a plant and measure whether certain inflammatory signals go up or down. Or they may feed a high dose of an extracted compound to animals. Or they may study an isolated substance from a food, not the food as you would actually eat it.
This is not bad science. This is often how science has to begin. If we want to understand whether a plant compound can influence inflammatory signaling, we need controlled experiments. A cell dish or animal model can help us understand mechanisms that would be impossible to study directly in humans at first.
But the problem starts when this early-stage research is translated too quickly into human advice.
There is a very big difference between saying “this compound reduced an inflammatory marker in immune cells in a dish” and saying “this food will reduce inflammation in your lipedema tissue.” Many things can disappear along the way. The dose may be unrealistic. The compound may not be absorbed well. The food matrix may change its effect. The person’s gut bacteria may transform it into something different. The inflammatory pathway studied in the lab may not be the pathway driving symptoms in a real human body.
This is why I become cautious when I see very confident claims about single foods.
Turmeric is a good example. Curcumin, the active compound often discussed in turmeric, has been studied intensely for its anti-inflammatory potential. It is biologically interesting. It may have effects in certain contexts. But curcumin is also poorly absorbed in the human body, and studies in humans are much more complex than the online claims suggest. Eating turmeric in food is not the same as taking a concentrated curcumin supplement, and neither of those is the same as exposing cells directly to curcumin in a laboratory.
The same applies to many other “superfoods.” Berries, green tea, olive oil, ginger, cocoa, grapes, herbs and spices may all contain compounds with interesting biological properties. But that does not make them universal medicine. A food can be nutritious and still not be a proven treatment. A compound can be promising and still not have strong evidence for your specific condition.
This distinction matters, especially for people with lipedema, because we are often vulnerable to oversimplified answers. Many of us have spent years not being believed, not being diagnosed, or being told that our painful tissue is just a weight problem. When someone finally gives us a clear list of what to eat, it can feel like relief. But clarity is not the same as truth.
The lipedema diet studies exist, but they do not give us a simple answer
There is now a small but growing cluster of studies looking at diet, inflammation and lipedema. That is important, and it is more than we had a few years ago. But these studies do not prove that there is one anti-inflammatory diet for everyone with lipedema.
They mostly point toward dietary patterns, not single foods.
Several studies have explored ketogenic diets, low-carbohydrate high-fat diets, Mediterranean-style diets and modified Mediterranean-ketogenic approaches. Some show improvements in body composition, pain, inflammatory markers or quality of life. That is promising. But the studies are still limited, often small, and sometimes come from the same research environments. They are useful, but they are not the same as a large, diverse, long-term evidence base.
One study is especially useful for understanding the difference between biomarkers and symptoms. In women with lipedema, a more pro-inflammatory diet score was associated with higher TNF-alpha and IL-6, two inflammatory markers measured in the blood. A higher Mediterranean Diet Score was associated with lower levels of those markers. On paper, that looks like a clean anti-inflammatory diet story.
But then comes the important part: in that study, the diet score was not significantly associated with pain scores or physical quality of life.
In other words, the blood markers moved with the diet pattern, but the things patients actually feel, such as pain and quality of life, did not clearly move with them in that study.
That does not make the study unimportant. It makes it more important. It shows us that “anti-inflammatory” cannot automatically be translated into “you will feel better.” Blood markers are useful, but they are not the whole disease. Lipedema pain may involve tissue pressure, fibrosis, nerves, vascular fragility, lymphatic load, central sensitization, hormones and mechanical factors. A cytokine in the blood may not capture all of that.
Other newer studies do report associations between more pro-inflammatory dietary patterns, ultra-processed food intake, pain, inflammatory markers and quality of life. So the symptom story is not absent. It is simply not settled. The evidence is early, cross-sectional in several cases, and unable to prove cause and effect. This is exactly why we need nuance.
A Mediterranean-style diet may be helpful for many people. A lower-carbohydrate or ketogenic approach may be helpful for some people. Reducing ultra-processed food may be a very sensible starting point. But none of this proves that all people with lipedema need the same diet, or that one food list can predict what will happen in your body.
The stronger evidence is about patterns, not magic foods
If there is one place where nutrition research is more useful, it is not in single foods. It is in dietary patterns.
A dietary pattern means the overall way you eat over time. Not one cup of green tea. Not one serving of berries. Not one spoon of olive oil. But the broader rhythm of your diet: how much fiber you eat, how much ultra-processed food you consume, how often you eat fish, whether most meals contain protein, how much refined sugar you eat, whether your carbohydrates are mostly whole or refined, whether you get enough micronutrients, and whether your meals keep your blood sugar relatively stable.
Anti-inflammatory dietary patterns often look similar to Mediterranean-style eating. They usually include vegetables, fruit, berries, legumes, whole grains if tolerated, fish, seafood, nuts, seeds, olive oil, herbs and other minimally processed foods. They are typically rich in fiber, unsaturated fats, polyphenols, minerals and other compounds that support metabolic and immune function.
On the other side, more pro-inflammatory dietary patterns are often characterized by high intake of ultra-processed foods, refined carbohydrates, sugar-sweetened drinks, low fiber intake, excess alcohol, frequent fried foods and large amounts of processed meats.
But even this needs nuance.
This does not mean that one dessert causes inflammation. It does not mean that white rice is poison. It does not mean that bread is always bad, or that everyone with lipedema must avoid dairy, gluten, fruit, potatoes or carbohydrates. The body does not judge foods morally. It responds biologically. And biology depends on context.
A slice of bread alone is not the same as a slice of bread with eggs, olive oil, vegetables and protein. Fruit alone is not the same as fruit eaten with Greek yogurt, chia seeds or nuts. Rice alone is not the same as rice eaten with fish, vegetables and fat. A dessert after a balanced meal is not the same as sugar on an empty stomach after a night of poor sleep.
The body responds to the whole meal, the amount, the timing, the person eating it and the biological state that person is in.
This is why the same food can feel fine one day and not fine another day. You may tolerate carbohydrates better after exercise than after several days of poor sleep. You may tolerate salty food differently in hot weather. You may react more strongly to alcohol before your period. You may find that certain foods trigger heaviness only when you are already stressed, inflamed, swollen or sleep deprived.
For people with lipedema, this is often very familiar. The tissue can feel more reactive in certain phases of life, certain phases of the cycle, or certain combinations of heat, hormones, stress and food. That does not mean you are imagining it. It means your body is not a simple machine.
Why the same food affects people differently
Even if a food truly has a mild anti-inflammatory effect in some people, the next question is still: why do some people notice a difference while others notice nothing?
One reason is the gut microbiome. Many plant compounds do not act in the body exactly as they exist in the food. They are transformed by bacteria in the gut. These bacteria help convert fibers and polyphenols into metabolites that may influence the immune system, gut barrier, vascular function and metabolism. But gut microbiomes vary enormously from person to person. Two people can eat the same food and produce different metabolites from it.
In a very real sense, the food does not become the same thing inside every body.
Genes also matter. Small genetic differences can influence how we absorb, transport, metabolize and respond to compounds in food. So can age, sex hormones, medication use, body composition, insulin sensitivity, physical activity and health status.
Dose matters too. Many lab studies use concentrations that are far beyond what we would ever reach through a normal meal. The effect of a purified compound at a high dose in a cell dish tells us very little about the effect of a cup of tea, a handful of blueberries or a spice used in cooking.
Then there is the rest of life. Sleep, stress, grief, trauma, economic pressure, social support, movement, pain and hormones are not separate from nutrition. They shape how the body responds to food. Food does not work in a vacuum. It works inside a life.
This is why I think we need to stop treating “anti-inflammatory” as a property that simply lives inside a food. It is more accurate to say that an anti-inflammatory effect may emerge in the meeting between a food, a gut microbiome, a metabolism, an immune system and a life context. That is a much less marketable sentence. But it is much closer to biology.
Supplements and “anti-inflammatory” treatments deserve the same skepticism
The same logic applies to supplements and treatments marketed toward inflammation or fibrosis.
Many compounds sound convincing because they have a plausible mechanism. They may influence inflammatory pathways in cells. They may affect fibrosis-related signaling. They may have antioxidant properties. They may make sense on paper. But plausible is not the same as proven.
Serrapeptase is one example. It has been promoted as an anti-inflammatory or antifibrotic enzyme, including after lipedema surgery. But a controlled study looking at serrapeptase after liposuction for lipedema did not find evidence strong enough to support routine use for fibrosis, pain or stiffness.
GLP-1 receptor agonists are another example. They are very interesting drugs, especially for metabolic disease, obesity and insulin resistance. They may have anti-inflammatory and antifibrotic effects in some biological contexts. But when it comes to lipedema itself, the direct evidence is still extremely limited. A small case series is not enough to conclude that these medications modify lipedema tissue.
Resveratrol is similar. It has interesting mechanisms related to inflammation, metabolism, estrogen signaling and oxidative stress. But for lipedema, much of the discussion remains mechanistic and speculative. It is not the same as evidence that taking resveratrol improves lipedema symptoms in real patients.
This does not mean these things are useless. It means we should place them in the right evidence category.
Interesting? Yes.
Worth studying? Yes.
A proven lipedema treatment? Not yet.
For a disease community that has been neglected for so long, this distinction is not pessimistic. It is protective.
The problem with universal food lists
The biggest problem with universal anti-inflammatory food lists is not that the foods are bad. Many of the foods on those lists are genuinely nutritious. I have nothing against berries, olive oil, fish, ginger, vegetables or green tea.
The problem is the certainty.
When foods are divided too neatly into “good” and “bad,” people often stop listening to their own bodies. A person may keep forcing themselves to eat something that gives them digestive distress because it is supposed to be anti-inflammatory. Another person may remove entire food groups they tolerate perfectly well because someone online said those foods are inflammatory. Someone else may feel guilty for eating rice, bread, dairy, fruit, potatoes or an occasional dessert, even though those foods may not be a problem for them at all.
This can become especially harmful in chronic illness communities, where people are already desperate for control.
Food fear is not anti-inflammatory. Chronic guilt is not anti-inflammatory. A diet that makes your life smaller, more anxious and more socially isolated is not necessarily healing, even if every ingredient on the plate looks perfect.
A more useful approach is to think in patterns and personal responses.
What happens when your meals contain enough protein? What happens when you reduce refined sugar? What happens when you eat more fiber? What happens when you drink alcohol several days in a row? What happens when you eat carbohydrates alone compared with carbohydrates in a balanced meal? What happens in the week before your period? What happens after poor sleep? What happens during travel, heat, grief, stress or hormonal treatment?
These questions are more useful than asking whether one food is officially anti-inflammatory.
What this means in practice
I do not want to replace one rigid list with another. That would defeat the point.
But I do think there are some gentle principles that make sense for many people with lipedema.
A good starting point is to build most meals from minimally processed foods. Make sure you get enough protein. Include vegetables, berries, fruit, legumes, grains or starches according to your own tolerance. Use fat sources such as olive oil, fatty fish, nuts, seeds, avocado or other foods that work for you. Pay attention to fiber, because fiber influences gut bacteria, blood sugar response, bowel function and the production of metabolites that may affect immune signaling.
Then look at the things that most often create problems for many people, even though not always for everyone: large amounts of refined sugar, sugar-sweetened drinks, frequent ultra-processed foods, heavy alcohol intake, very low fiber intake and meals that create large blood sugar swings.
For some people with lipedema, lowering carbohydrate intake may be useful. For others, it may be enough to change carbohydrate quality and meal composition. Some may feel best with a ketogenic approach. Others may feel better with a Mediterranean-style diet that includes legumes, fruit, oats, potatoes or whole grains. Some tolerate dairy. Some do not. Some tolerate gluten. Some do not. Some react strongly to sugar. Others react more to alcohol, heat, lack of sleep or hormonal changes.
The point is not to find the strictest diet. The point is to find the most supportive pattern.
A symptom diary can be helpful, but only if it is used calmly. The goal is not to obsess over every bite. The goal is to notice patterns over weeks and months. What did you eat? How did you sleep? Where are you in your cycle? How stressed were you? How did your legs feel that evening and the next day? Did you feel swelling, heaviness, pain, pressure, cravings, fatigue or digestive symptoms?
Over time, patterns often become clearer.
Maybe gluten is not the issue, but large amounts of white bread without protein are. Maybe dairy is not the issue, but ice cream with sugar is. Maybe carbohydrates are not the issue, but fast carbohydrates alone are. Maybe you tolerate wine occasionally, but not in heat, not before your period and not after poor sleep. Maybe fruit is fine, but candy is not. Maybe your body handles rice well after strength training, but poorly after a sedentary day.
This is not about perfection. It is about learning.
Anti-inflammatory eating should not make your life smaller
I think one of the most important things we can say in the lipedema community is this: food should support the body, not become another source of punishment.
Many people with lipedema have already been blamed for their bodies. They have been told to lose weight, exercise more, try harder, eat less, be more disciplined. They have lived with pain that others could not see, tissue changes that were dismissed, and symptoms that were reduced to lifestyle.
So when we talk about food, we need to be careful.
Yes, nutrition matters. Yes, food can influence inflammation markers, blood sugar, fluid balance, gut function and symptoms. Yes, many people with lipedema do notice clear food triggers. I believe those experiences should be taken seriously.
But we should not turn nutrition into another moral test.
An anti-inflammatory way of eating is not just about what is missing from your plate. It is also about whether the pattern is sustainable, nourishing, flexible, socially possible and emotionally safe. A diet you can live with for years will usually be more useful than a perfect protocol you can follow for three weeks while feeling miserable.
For people with lipedema, the goal is not to eat like a machine. The goal is to reduce pain, support tissue health, protect metabolic health and still have a life.
“Anti-inflammatory food” is not one recipe.
And it is certainly not one universal recipe for lipedema.
There are anti-inflammatory dietary patterns. There are foods that contain compounds with interesting biological properties. There are nutrients that support immune regulation, vascular function, gut health and metabolic stability. There are also food patterns that may worsen blood sugar swings, gut symptoms, fluid retention or systemic inflammatory burden in some people.
The lipedema research makes the story more complicated, not less
Lipedema tissue is not simply ordinary inflamed fat. Its immune profile may differ from obesity. M2-like macrophages, fibrosis, tissue remodeling, pain and possible metabolic protection can all exist in the same conversation. A diet can be associated with lower inflammatory markers in blood without clearly improving pain or quality of life in every study. And a promising mechanism is not the same as a proven treatment.
So no, there is no single anti-inflammatory food list that works the same way for every person with lipedema. The same food can help one person, do nothing for another and trigger symptoms in a third. That does not mean anyone is doing it wrong. It means biology is personal.
For lipedema, this is not a disappointing conclusion. It is a freeing one. You do not have to chase every online list. You do not have to fear every food someone calls inflammatory. You do not have to copy another person’s diet to prove that you are taking your condition seriously.
You can begin with the science, stay honest about what we do not yet know, and then carefully observe your own body. Because the most useful anti-inflammatory diet is not the one that looks best on paper. It is the one that helps your body feel calmer, without making your life smaller.
Welcome to LipedemaScience.com!